HCV Treatment Process, AL DOC, 2004
Download original document:
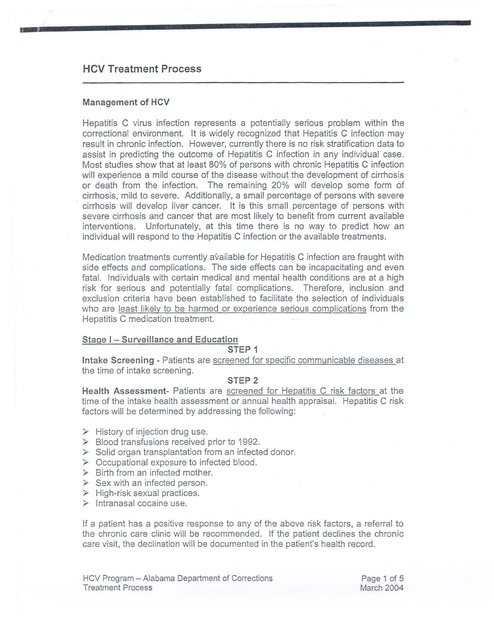
Document text
Document text
This text is machine-read, and may contain errors. Check the original document to verify accuracy.
, HCV Treatment Process Management of HCV Hepatitis C virus infection represents a potentially serious problem within the correctional environment. It is widely recognized that Hepatitis C infection may result in chronic infection. However, currently there is no risk stratification data to assist in predicting the outcome of Hepatitis C infection in any individual case. Most studies show that at least 80% of persons with chronic Hepatitis C infection will experience a mild course of the disease without the development of cirrhosis or death from the infection. The remaining 20% will develop some form of cirrhosis, mild to severe. Additionally, a small percentage of persons with severe cirrhosis will develop liver cancer. It is this small percentage of persons with severe cirrhosis and cancer that are most likely to benefit from current available interventions. Unfortunately, at this time there is no way to predict how an individual will respond to the Hepatitis C infection or the available treatments. Medication treatments currently available for Hepatitis C infection are fraught with side effects and complications. The side effects can be incapacitating and even fatal. Individuals with certain medical and mental health conditions are at a high risk for serious and potentially fatal complications. Therefore, inclusion and exclusion criteria have been established to facilitate the selection of individuals who are least likely to be harmed or experience serious complications from the Hepatitis C medication treatment. Stage I Surveillance and Education STEP 1 Intake Screening - Patients are screened for specific communicable diseases at the time of intake screening. STEP 2 Health Assessment Patients are screened for Hepatitis C risk factors at the time of the intake health assessment or annual health appraisal. Hepatitis C risk factors will be determined by addressing the following: A ;.> History of injection drug use. ;.> Blood transfusions received prior to 1992. }> }> }> ;.> ;.> ;.> Solid organ transplantation from an infected donor. Occupational exposure to infected blood. Birth from an infected mother. Sex with an infected person. High-risk sexual practices. Intranasal cocaine use. If a patlent has a positive response to any of the above risk factors, a referral to the chronic care clinic will be recommended. If the patient declines the chronic care visit, the declination will be documented in the patient's health record. HCV Program - Alabama Department of Corrections Treatment Process Page 1 of 5 March 2004 STEP 3 Chronic Care Scheduled Visit - The chronic care encounter will be scheduled to take place within 90 days of the health assessment. Patients will receive education and counseling and may be offered a screening test for Hepatitis C, based on a more comprehensive assessment of risk factors and medical appropriateness. The HCV Patient Information/Education document is signed by the patient and provider. (Attachment A) STEP 4 Hepatitis C Antibody Testing The Hepatitis C antibody test is recommended for screening and is sufficient to exclude a diagnosis of chronic Hepatitis C infection in most individuals with intact immune systems. A false negative Hepatitis C antibody test may occur in a small number of inmates who are immune-deficient (Le., HIV/AIDS). In patients with immune deficiency who have an elevated ALT (indicating possible Hepatitis e infection) and a negative Hepatitis e antibody test, a Hepatitis e RNA polymerase chain reaction (PCR) should be performed. v STEP 5 Hepatitis C Antigen Testing -It has been demonstrated that approximately 10 to 15% of patients who contract Hepatitis C will spontaneously clear the virus. A peR HCV RNA antigen test will be completed. If the test is positive the evaluation will continue. If the test is negative, the patient should be instructed to have the test repeated in five years. STEP 6 Hepatitis A & B Vaccine - Patients who are HeV antibody positive will be offered the Hepatitis A and B vaccines as indicated. » » Administer Hepatitis A Administer vaccinated Hepatitis A vaccine series unless it is known that the patient has disease or previous vaccination. Hepatitis B vaccine series unless the patient was previously or serology indicates previous infection. Stage II - Eligibility for Medication Treatment STEP 1 Baseline eligibility screening will be done pursuant to the comprehensive surveillance, educational and vaccination program in Stage 1. Eligibility will be considered for inmates that have at least a 24-month sentence remaining. The reason for stipulating this minimum length of time is because: 1. Complex and time-consuming educational and clinical evaluation requirements, 2. Adherence to treatment is essential to maximize successful outcomes, and 3. Side effects should be monitored for at least 6 months post treatment. Hev Program - Alabama Department of Corrections Treatment Process Page 2 of 2 March 2004 STEP 2 Consent and Education Attestation - The patient will review and sign the HCV Patient/Education Information document. (Attachment A) The patient will review and sign the HeV Evaluation and Treatment Consent form in the "determining eligibility" section. (Attachment C) CDC patient education material will also be used to provide inmates with a more complete understanding of the disease process. STEP 3 Determining Eligibility - Patients with the conditions listed as absolute exclusion criteria will be excluded from the eligibility pool because the risks outweigh the benefits of therapy. Following is a list of absolute and relative exclusion criteria. Patients who have an absolute exclusion criteria will not have further evaluation or testing unless the condition(s) resolves or improves (example pregnancy and anemia) in which case they will be reevaluated within 90 days of resolution. Absolute Exclusion Criteria o o o o o o Ages 180r~60 Remaining incarceration time ~ 24 months. Presence of an Axis I diagnosis that is not controlled and stable as determined by the treating psychiatrist. History of solid organ transplant. Presence or history of an autoimmune disorder. Presence or history of decompensated cirrhosis, presence or history of ascites or encephalopathy (albumin S 3.2 gm/dl, biiirubin > 3.0 gm/dl). results outside acceptable limits (Hgb ~ 12 females, ~ 13 for males; WBC > 3,000; ANC S 1,500 & platelets S 100,OOO/mm). Creatinine ~ 1.7 or creatinine clearance::. 50 mJlminute. Normal ALT «2.0 times normal at 0,3 and 6 months). Positive pregnancy test. Active TB Auto Immune Disease e.g. - Lupus, Graves Disease, R.A., M.S., Myasthenia Gravis Cancer - not in remission Hemoglobinopathies o esc o o o o o o o "No further evaluation should be completed so long as the absolute criterion exists." HCV Program - Alabama Department of Corrections Treatment Process Page 3 of 5 March 2004 Relative Exclusion Criteria o o o o o o o o o o o o o o o Hepatitis B Co-infection Diabetes - poorly controlled with Hgb. A1C ~ 9.0 Ischemic Cardiac Disease or Cerebrovascular Disease Hypertension - poorly controlled CHF Peripheral Vascular Disease - Symptomatic COPD - severe Seizures - poorly controlled Active Thyroid Disease Active Gout Significant CNS Trauma - recent within the past six months Poor adherence to treatment including ~ 80% of clinic visits and medications, to the extent the inmate made the choices. Alcohol and illicit drug use within one year. Interferon/Ribavirin sensitivity. Ufe expectancy < 10 years. The provider is required to review relative exclusion criteria with the Regional Medical Director prior to proceeding with further evaluation. STEP 4 Liver Biopsy - Liver biopsy provides a unique source of information on fibrosis - and assessment of histology. The information obtained on liver biopsy allows affected individuals to make a more informed choice about the initiation or postponement of antiviral treatment. Thus, the liver biopsy is a useful part of the informed consent process. In general, a baseline assessment of liver histology offers a valuable standard for subsequent comparisons. However, the appropriate interval for sUbsequent evaluations is yet to be determined. A biopsy will be required prior to initiating medication for patients with Hepatitis C viremia with genotype 1A or 1B. A biopsy will not be required for genotypes 2, 3 & 4 and for patients with compensated cirrhosis. Stage III - Medication Treatment The provider will initiate a treatment plan including medication treatment if the patient is determined to be eligible and the patient consents for medical treatment by signing patient education document and the HCV consent form in the medication initiation section. HCV Disease: Evaluating patient new to a facility on medication for HCV disease HCV Program - Alabama Department of Corrections Treatment Process Page 4 of 5 March 2004 Patients arriving at a ADOC facility, either from the community or another ADOC facility, who are on antiviral therapy for HCV disease will be evaluated within 72 hours for consideration of continuing or resuming medication therapy. There should be a low threshold for continuing the medication for the first week while evaluating the appropriateness of the medication regimen. As a part of this evaluation, patients should be reviewed for the following: 1. Absolute exclusion criteria (but not the minimum remaining sentence since they have already been on therapy). 2. Response to therapy as measured by viral load. 3. Dosing adjustment due to anemia. 4. Adherence Continuing Therapy Patients who are already on a potent antiretroviral regimen and who are adherent to therapy should have the HVC medications continued by the physician during the intake process. A complete medical record review and clinic visit should be done within one week to review: 1. Medication adherence 2. Response to therapy 3. Medication side effects 4. Assure patient education material has been reviewed and consent forms signed. Resuming Therapy Patients who are non·adherent to therapy or who have had an interruption in medication for greater than 2 weeks should be evaluated in consult with the State Medical Director prior to restarting antiretroviral therapy. If there is any question about the adherence pattern the treatment should be continue for a week while the information is being reviewed. HCV Program - Alabama Department of Corrections Treatment Process Page 50f 5 March 2004 Attachment A HCV • Patient Information/Education Adopted from the Schering~Plough medication guide and labeling document. HEPATITIS C VIRUS The Hepatitis C virus can and does damage the liver. However, the majority of patients never experience symptoms while others can take from 10 to 15 years before symptoms develop. The damage caused by the Hepatitis C virus may range from none to mild, moderate or life threatening. Symptoms may include: » » » }> » Fatigue Jaundice (yellowing of the eyes) Nausea Pain in the abdomen Fever >- » » » » Muscle Aches Joint Pain Loss of appetite Diarrhea Vision Loss HEPATITIS C TREATMENT At the present time there is a medication treatment strategy that is FDA approved for the treatment of the Hepatitis C infection: Pegylated Interferon and Ribavirin combination treatment. Patients are treated for 24-48 weeks and are followed for 24 weeks post-treatment. The goal of treatment is to achieve sustained virologic clearance. Response to treatment is defined as undetectable HCV RNA and normalization of ALT at 24 weeks posltreatment. It is important to note that there is no data regarding whether Pegylated Interferon treatment will prevent transmission of HCV infection to others. Additionally, it is not known if treatment with Pegylated Interferon will cure Hepatitis C or prevent cirrhosis, liver failure, or liver cancer that may be the result of infection with the Hepatitis C virus. Approximately 10-14% of patients discontinued treatment due to side effects. It is recommended that patients receiving Pegylated Interferon, alone or in combination with Ribavirin, be discontinued from treatment if HCV viral levels do not show an improvement at 12 weeks or are absent at 24 weeks. INDICATIONS Pegylated Interferon is a treatment for some people who are infected with the Hepatitis C virus. However, Pegylated Interferon/Ribavirin combination treatment can have serious side effects that may cause death. Therefore the treatment is not for everyone. Prior to beginning treatment, patients should discuss the risks and benefits so that they are prepared to make an informed decision. CONTRAINDICATIONS Pegylated Interieron/Ribavirin combination treatment is contraindicated in: » Paiients with hypersensitivity to ribavirin or any other component of the product. HCV Program - Alabama Department of Corrections Patient Education Information Page 1 of 4 April 2003 >>.>- » » Women who are pregnant, planning to become pregnant or are breast-feeding. Men whose female partners are pregnant. Patients that have Hepatitis Caused by your immune system attacking your liver or unstable liver disease. Patients that have abnormal red blood cells such as sickle-cell anemia or thalassemia major. Patients with a history of significant or unstable cardiac disease should not be treated with Pegylated Interferon/Ribavirin combination treatment. Serious consideration and thought should occur before Interferon/Ribavirin, is you have any of the following conditions: taking Pegylated Conditions that rna effect Treatment Alcoholism Deoression or anxiety Orua abuse or addiction Hioh blood Dressure Previous heart attack, or heart oroblems Anv kind of autoimmune disease Liver oroblems other than Heoatitis C Heoatitis B infection Thvroid Droblems HIV infection SleeD Droblems Diabetes Colitis Cancer Kidnev oroblems Bodv oraan transDlan!s Bleeding problems SIDE EFFECTS Patients may present with side effects within the first 12 weeks of treatment and many continue to experience adverse events several months after discontinuation of treatment. In the combination treatment trial, dose reductions due to adverse reactions occurred in 42% of patients receiving Pegylated Interferon. In the Pegylated Interferon/Ribavirin combination trial the most common adverse events were psychiatric which occurred among 77% of the patients and included most commonly depression, irritability, and insomnia. Pegylated Interferan/Ribavirin induced fatigue or headache was also found in approximately two-thirds of patients and induced fever or rigors in approximately half of the patients. Following is a description of the side effects experienced by patients taking Interferon/Ribavirin treatment. Mental Health And Suicide - Pegylated Interferon/Ribavirin therapies may cause mood and behavior problems. Behavioral problems include irritability and depression. Some patients become more aggressive and some think about hurting or killing themselves or others. Heart Problems - Some patients taking Pegylated Interferon/Ribavirin therapies may develop problems with low blood pressure, fast heart rate and very rarely, heart attacks. Hev Program - Alabama Department of Corrections Patient Education Information Page 2of4 April 2003 Blood Problems· Pegylated Interferon/Ribavirin therapies commonly lower two types of blood cells, white blood cells and platelets. The therapies have also been shown to decrease red blood cells, resulting in anemia. Anemia can be dangerous, especially if a person has heart or circulatory problems. Body Organ Problems - Pegylated lnteneron/Ribavirin therapies have been shown to cause damage to internal organs. Symptoms of severe abdominal pain can indicate internal organ damage. Birth Defects - Ribavirin may cause birth defects and/or death of the unborn child. Extreme care must be taken to avoid pregnancy in female patients and in female partners of male patients. Endocrine Disorders - Pegylated Inteneron causes or aggravates hypothyroidism and hyperthyroidism. Hyperglycemia has been observed in patients treated with Pegylated Interferon. Diabetes mellitus has been observed in patients treated with alpha interferons. Colitis • Fatal and nonfatal ulcerative or hemorrhagic/ischemic colitis have been observed within 12 weeks of the start of alpha interferon treatment. Abdominal pain, bloody diarrhea, and fever are the typical manifestations. The colitis usually resolves within 1~3 weeks of discontinuation of alpha interferons. Autoimmune Disorders - Pegylated Interferon treatment may cause the development or exacerbation of autoimmune disorders such as thrombocytopenia, rheumatoid arthritis, systematic lupus, and psoriasis. Pancreatitis - Fatal and nonfatal pancreatitis has been observed in patients treated with alpha interferon. Pegylated Interferon treatment should be suspended in patients with signs and symptoms suggestive of pancreatitis and discontinued in patients diagnosed with pancreatitis. Common, Less Serious Side Effects Flu symptoms: Appetite: Thyroid: Skin reactions: Hair Thinning: Including headache, muscle aches, tiredness and fever. Including nausea, loss of appetite, and weight loss. Some patients develop changes in the function of their thyroid. Symptoms include inability to concentrate, feeling cold or hot all the time, a change in weight and skin changes. Redness, swelling, and itching are common at the injection site. Hair loss stops and hair growth returns after treatment is stopped. On-Going Side Effects A stUdy showed that by the end of the 6·month follow-up period the incidence of ongoing adverse events by body class in the PEG-INTRON 1.5/REBETOL groups was: ~ 33% (psychiatric), ~ 20% (musculoskeletal), and HCV Program - Alabama Department of Corrections Patient Education Information Page 3 of 4 April 2003 } 10% (for endocrine and for GI). In addition, approximately 10-15% of patients weight loss, fatigue and headache had not resolved. DOCUMENTATION OF EDUCATION Education Session 1 • Screening I understand that I have risk factors for Hepatitis C. I have been provided with the HCVPatient Information/Education material is adapted from the ~Medication Guide" established by Schering-Plough Research Institute. The information in this document has been reviewed with me and I have that the opportunity to ask questions. PATIENT'S SIGNATURE DATE SIGNED PROVIDER'S SIGNATURE DATESIG:-.lED Education Session 2 - HCV Positive I understand that I have tested positive for the Hepatitis C virus. I have been provided with the HeV-Patient Infannatien/Education material is adapted from the "Medication Guide- established by Schering·Plough Research Institute. The information in this document has been reviewed with me and I have that the opportunity to ask questions. PATIENT'S SIGNATURE DATE SIGNED PROVIDER'S SIGNATURE DATE SIGNED Education Session 3 - Treatment I understand that I am eligible to receive Interferon/Ribavirin treatment. I have been provided with the HCV·Patient Information/Education material is adapted from the "Medication Guide" established by Schering-Plough Research Institute. The information in this document has been reviewed with me and I have that the opportunity to ask questions. PATIENT'S SIGNATlJRE DATE SIGNED PROVIDER'S SIGNATURE DATE SIGNED HCV Program - Alabama Department of Corrections Patient Education Information Page 4 of 4 April 2003 Attachment B Hev - Provider Reference Adopted from the Schering-Plough medication guide and labeling document. HEPATITIS C VIRUS The hepatitis C virus can and does damage the liver. However, the majority of patients may never experience symptoms while others can take from 10 to 15 years before symptoms develop. The damage caused by the hepatitis C virus may be minimal or severe. Symptoms may include: » » Fatigue Jaundice (yellowing ofthe eyes) Nausea >- Pain in the abdomen );> Fever » >- Muscle Aches Joint Pain Loss of appetite :> Diarrhea :> Vision Loss >- » HCV TREATMENT At the present time there is a medication treatment strategy that is FDA approved for the treatment of the Hepatitis C infection: Pegylated Interferon and Ribavirin combination treatment. Patients are treated for 24-48 weeks and are followed for 24 weeks post-treatment. The goal of treatment is to achieve sustained virologic clearance. Response to treatment is defined as undetectable HCV RNA and normalization of ALT at 24 weeks posttreatment. It is important to note that there is no data regarding whether Pegylated Interferon treatment will prevent transmission of HCV infection to others. Additionally, It is not known if treatment with Pegylated Interferon will cure Hepatitis C or prevent cirrhosis. liver failure, or liver cancer that may be the result of infection with the Hepatitis C virus. Approximately 10-14% of patients discontinued treatment due to side effects. It is recommended that patients receiving Pegylated Interferon, alone or in combination with Ribavirin, be discontinued from treatment if HCV viral levels remain high after six months of treatment. INDICATIONS Pegylated Interferon, peginterferon alfa-2b, is indicated for use alone or in combination with REBETOL (ribavirin, USP) for the treatment of chronic hepatitis C in patients with compensated liver disease who have not been previously treated with interferon alpha and are at least 18 years of age. However, Pegylated lnterferon/Ribavirin combination treatment can have serious side effects that may cause death. Therefore the treatment is not for everyone. Prior to beginning treatment, patients should discuss the risks and benefits so that they are prepared to make an informed decision. HCV Program - Alabama Department of Corrections Provider Reference Page 1 of 5 April 2003 CONTRAINDICATIONS Pegylated Interferon/Ribavlrin combination treatment is contraindicated in: );> );> » }> » » Patients with hypersensitivity to ribavirin or any other component of the product. Women who are pregnant, planning to become pregnant or are breast-feeding. Men whose female partners are pregnant. Patients that have hepatitis caused by your immune system attacking your liver or unstable liver disease. Patients that have abnormal red blood cells such as sickle-cell anemia or thalassemia major. Patients with a history of significant or unstable cardiac disease should not be treated with Pegylated Interferon/Ribavirin combination treatment. Serious consideration and thought should occur before Interferon/Ribavirin, is you have any of the following conditions: taking Pegylated Conditions that may effect Treatment Depression or anxiety Alcoholism Hiqh blood pressure Druq abuse or addiction Previous heart attack, or heart problems Any kind of autoimmune disease Liver problems other than Hepatitis C Hepatitis B infection Thyroid oroblems HIV infection Diabetes Sleeo problems Colitis Cancer Kidney oroblems Body oroan transolants Bleedin roblems SIDE EFFECTS Patients may present with side effects within the first 12 weeks of treatment and many continue to experience adverse events several months after discontinuation of treatment. In the combination treatment trial, dose reductions due to adverse reactions occurred in 42% of patients receiving Pegylated Interferon/Ribavirin. In the Pegylated I nterferon/Ribavirin combination trial the most common adverse events were psychiatric which occurred among 77% of the patients and included most commonly depression, irritability, and insomnia. Pegylated Interferon/Ribavirin induced fatigue or headache was also found in approximately two-thirds of patients and induced fever or rigors in approximately half of the patients. Following is a description of the side effects experienced by patients taking Interferon/Ribavirin treatment. HCV Program - Alabama Department of Corrections Provider Reference Page 2 of 5 Apnl2003 Mental Health And Suicide - Pegylated Interferon/Ribavirin therapies may cause mood and behavior problems. Behavioral problems include irritability and depression. Some patients become more aggressive and some think about hurting or killing themselves or others. Heart Problems - Some patients taking Pegylated Interferon/Ribavirin therapies may develop problems with low blood pressure, fast heart rate and very rarely, heart attacks. Blood Problems - Pegylated Interferon/Ribavirin therapies commonly lower two types of blood cells, white blood cells and platelets. The therapies have also been shown to decrease red blood cells, resulting in anemia. Anemia can be dangerous, especially if a person has heart or circulatory problems. Body Organ Problems - Pegylated Interferon/Ribavirin therapies have been shown to cause damage to internal organs. Symptoms of severe abdominal pain can indicate internal organ damage. Birth Defects - Ribavirin may cause birth defects and/or death of the unborn child. Extreme care must be taken to avoid pregnancy in female patients and in female partners of male patients. Endocrine Disorders - Pegylated Interferon causes or aggravates hypothyroidism and hyperthyroidism. Hyperglycemia has been observed in patients treated with Pegylated Interferon. Diabetes mellitus has been observed in patients treated with alpha interferons. Colitis - Fatal and nonfatal ulcerative or hemorrhagic/ischemic colitis have been observed within 12 weeks of the start of alpha interferon treatment. Abdominal pain, bloody diarrhea, and fever are the typical manifestations. The colitis usually resolves within 1-3 weeks of discontinuation of alpha interferons. Autoimmune Disorders - PegyJated Interferon treatment may cause the development or exacerbation of autoimmune disorders such as thrombocytopenia, rheumatoid arthritis, systematic lupus, and psoriasis. Pancreatitis - Fatal and nonfatal pancreatitis has been observed in patients treated with alpha interferon. Pegylated Interferon treatment should be suspended in patients with signs and symptoms suggestive of pancreatitis and discontinued in patients diagnosed with pancreatitis. Common, Less Serious Side Effects Flu symptoms: Appetite: Thyroid: Blood Sugar: Including headache, muscle aches, tiredness and fever. Including nausea, loss of appetite, and weight loss. Some patients develop changes in the function of their thyroid. Symptoms include inability to concentrate, feeling cold or hot all the time, a change in weight and skin changes. Some patients may develop diabetes. HCV Program - Alabama Department of Corrections Provider Reference Page 3 of 5 Aprl'2003 Skin reactions: Hair Thinning: Redness, swelling, and itching are common at the injection site. Hair loss stops and hair growth returns after treatment is stopped. On-Going Side Effects A study showed that by the end of the 6-month follow-up period the incidence of ongoing adverse events by body class in the PEG-INTRON 1.5/REBETOL groups was: » » » 33% (psychiatric), 20% (musculoskeletal), and 10% (for endocrine and for GI). In addition, approximately 10-15% of patients weight loss, fatigue and headache had not resolved. MONITORING It is recommended that patients receiving Pegylated Interferon, alone or in combination with ribavirin, be discontinued from treatment if HCV viral levels remain high after 6 months of treatment. Pegylated Interferon treatment should be suspended in patients with signs and symptoms suggestive of pancreatitis and discontinued in patients diagnosed with pancreatitis. Patients were treated for 48 weeks and were followed for 24 weeks post-treatment. Patients should receive an eye examination at baseline. Patients with preexisting ophthalmologic disorders (e.g. diabetic or hypertensive retinopathy) should receive periodic ophthalmologic exams during interferon alpha treatment. Any patient who develops ocular symptoms should receive a prompt and complete eye examination. Pegylated Interferon treatment should be discontinued in patients who develop new or worsening ophthalmologic disorders. Patients should undergo monthly pregnancy tests during treatment and for six months posHreatment. OUTCOME Mono-therapy - A randomized study compared treatment with Pegylated Interferon to treatment with lNTRON A. The patients were not previously treated with interferon alfa, had compensated liver disease, detectable HCV RNA, elevated ALT, and liver histopathology consistent with chronic hepatitis. Patients were treated for 48 weeks and were followed for 24 weeks post~treatment. HCV Program - Alabama Department of Corrections Provider Reference Page 4 of 5 April 2003 Response to treatment is defined as undetected HCV RNA and normalization of ALT levels at 24 weeks post treatment. Response rates to the 1.0 and 1.5 ~g/kg Pegylated Interferon doses were similar (approximately 24%) to each other and were both higher than the response rate to INTRON A (12%). Patients infected with HCV genotype 1, and patients with high baseline levels of HCV RNA (more than 2 million copies per ml of serum); were less likely to respond to treatment with Pegylated Interferon. Patients receiving PegyJated Interferon with genotype 1 had a response rate of 14% while patients with other viral genotypes had a 45% response rate. Ninety-six percent of the responders in the Pegylated Interferon groups and 100% of responders in the INTRON A group first cleared their viral RNA by week 24 of treatment. Combination Treatment - A randomized study compared treatment with two PEG· Intran/REBETOL regimens [PEG-Introm 1.5 ~g/kg SC once weekly (QW)/REBETOL 800 mg PO daily (in divided doses); PEG-Intran 1.5 ~g/kg SC QW for 4 weeks then 0.5 ~g/kg SC QW for 44 weeks/REBETOL 1000/1200 mg PO daily (in divided doses)] with INTRON A (3 MIU SC thrice weekly (TIW)/REBETOL 1000/1200 mg PO daily (in divided doses). Response to treatment is defined as undetected HCV RNA and normalization of ALT levels at 24 weeks post treatment. The response rate to the PEG-Intron 1.5 Ilg/kg plus ribavirin 800 mg dose was higher that the response rate to INTRON AlREBETOL. The response rate to PEG-Intran 1.5 ---+ 0.5 ).lg/kg/REBETOL was essentially the same as the response to INTRON AlREBETOL, Patients with viral genotype 1, regardless of viral load, had a lower response rate to PEG-Intran (1.5 mg/kg)/REBETOL compared to patients with other viral genotypes. Patients with both poor prognostic factors (genotype 1 and high viral load) had a response rate of 30% (78/256) compared to a response rate of 29% (71/247) with INTRON AlREBETOL. Attachment C HCV Evaluation and Treatment Consent Form ===,- 1 'ATltJ','T'$ NAME _ ID I"UMB£R consent to the evaluation and polential medication adminisrration, or continuation of a current tteatment regimen initiated outside of this facility, for Hepatitis C based on the information provided, explaining the risks and polential benefits consistent with the manufacturer's recommendations. I understand that treatment consists of injections of an interferon product up to three times per week and may include ribavirin pills 10 be taken two times daily for 6 to 12 months. I understand that treatment also involves multiple visits to obtain blood for laboratory testing necessary for ongoing monitoring. I understand that there is no data regarding whether interferon product treatmem will prevent transmission of Hepatitis C vinls to others. Also, it is not known if treattnenl with an interferon product will cure Hepatitis C or prevent cirrhosis, liver fail~, or liver cancer that may be the result of infection with the Hepatitis C virus. Funhennore, I understand that even If the Hepatitis C treatment is successful in eliminating the vina, if I engage in high-risk behaviors, I may become re-infected with Hepatltis C. Currently, an interferon product and nbavirin combination treatment represents the best option for clearing the virus from your blood. Many patients do not respond to this treatment. if you do not respond the medications will be discontinued. Treatment for Hepantis C may have serious side effecTS, including wonening of liver inflammation, anemia, all~rgic reaction, hean attack, severe depression, suicide, pneumonia, loss of vision, or thyroid disease. Most people who aJe treated for Hepatitis C have flu-like symptoms that are sometimes very uncomfonable. These symptoms include fever, headache, chills, sore muscles, fatigue, nausea, vomiting, diarrhea and loss ofappetile. Approximately 10% to 15% ofpeople receiving this t'eatment Stop because of side effecTS. The side effects, however, can be severe enough to result in death. Binh defects may occur if either parent is undergoing treatment for Hepatitis C al the time or within six months before a pregnancy begins. Compliance is an essential component of the treatmenl for Hepatitis C. I understand that I must follow !he established treatment plan and that treatment may be discontinued if! do not comply. TreaDnenl consists of directly obsenred therapy. I understand that I should not initiate a pregnancy during or for at least six months following treatment. Female patients should use two forms of binh control during treatment and for 6 months following treatment. Males should use a condom and inform female partners of the need for a second form of contraception. Should you be released during the medication phase of your treatment it is extremely important that you establish a physician patient relationship with a specialist in the treatment of Hepatitis C. It is also imponant that you comply with tbe necessary life style changes to include not using illegal drugs or practicing unsafe sex. DETERMINING ELIGTRILITY Cl Not applicable. Patient admitted on treatment and eligihility verified. o I consent to eligibility testing to include blood tests and x-ray studies as well as a liver biopsy. I understand that J may withdraw or cancel this consent in writin at any time. PATIENT'S SIGNATURE DATE SIGNED PROVIDER'S SIGNATURE DATE SIGNED INITIATION/CONTINUAnON OF MEDICATION TREATMENT o I consent to medication treatment 10 include an interferon product and Ribavirin. I understand that I may withdraw or cancel this consent in writin al an time. PATIENT'S SIGNATURE DATE SIGNED PROVIDER'S SIGNATURE DATE SIGNED DECLlI'\E PARTICIPATION o fu"",. I decline evaluation or medication treatment at this time (circle one). I undentznd that I may requ~SI treattnent PATiENT'S SIGNATURE DATE SIGNED WfIl','ESS'SIGNATURE DATE SIGNED Hev Program - Alabama Depanment of Corrections Treatment Consent Form in the March 2004 Attachment D Hev Evaluation & Referral Flow Sheet [ID NUMBER PATIENT NAME ~ ; " ~ '" I DATE I FACILITY Patient is positive for the Hepatitis C virus. (Quantitative HeV obtained.) Patient given Schering-Plough or Pegasys "Medication Guide," as appropriate. Provider educates patient on Hepatitis C infection and treatment The education has been documented. 0 0 DATE: PROVIDER SIGNATURE: Initiate eligibility process 0 Patient signed Infonned Consent or refusal for detennining eligibility for InterferonJRibavirin treatment. .~ 0 Obtain labs as required to determine eligibility. (If no other absolute exclusion criteria are present.) '" ~ '" DATE: PROVIDER SIGNATURE: Relative Exclusion Criteria ** Ahsolute Exclusion Criteria* 0 0 0 0 Age~ Igor~60 0 Remaining incarceration time ~ 24 months. 0 Presence of an Axis I diagnosis that is!!2! controlled and stable as determined by the treating psychiatrist. 0 History of solid organ transplant. 0 Presence or history of an autoimmune disorder. 0 Presence or history or decompensated cirrhosis, presence or history of ascites or encephalopathy (albumin.5. 3 2 gmldl, bilirubin:> 3.0 gmldl). 0 CBe results outside acceptable limits (Hgb.::: 12 females, .5. 13 for males; WBC > 3,000; ANC,::: 1,500 & platelets '"~ '"- 0 0 0 0 0 • 0 0 0 0 0 0 0 0 :::: 100,000/mm). Creatinine?: 1.7 or creatinine clearance:::: 50 ml/minute. Normal ALT «2.0 times normal at 0, 3 and 6 months). Positive pregnancy test. Active TS Auto Immune Disease e.g. - Lupus, Graves Disease, R.A., M.S., Myasthenia Gravis 0 Cancer - not in remission o Hemoglobinopathies "No further evaluation should be completed so long as the absolute criterion exists." 0 Hepatitis B Co-infection Diabetes - poorly controlled with Hgb. A I C ~ 9.0 Ischemic Cardiae Disease oc Cerebrovascular Disease Hypertension - poorly controlled CHF Pcripheral Vascular Disease - Symptomatic COPD - severe Seizures - poorly controlled Active Thyroid Disease Active Gout Significant CNS Trauma - recent within the past six months 0 Poor adherence to treatment inclUding ~ 80% of clinic visits and medications, to the extent the inmate made the choices. 0 Alcohol and illicit drug use within one year. 0 Interferon/Ribavirin sensitivity. Life expectancy < 10 years. ··The provider is required to review relative exclusion criteria with the Regional Medical DirectOr prior to proceeding with further evaluation. ; Non-Formulary Request for Genot)'pe Testing 0 Obtain HCV genotype. Provider submits Non-formulary Lab Request fonn with a copy ofthis form to the Regional Medical Director. Approval must be received prior to ordering tests. '" STAFF SIGNATURE: ~ '"~ DATE: Risk Stratification and Treatment Options 0 Provider reviews test results with patient to detetmine risk stratifications and therapeutic options. 0 Provider submits an Outpatient RMD Consultation fonn for a liver biopsy, if indicated, with a copy of this fonn to the Regional Medical Director. Approval must be received prior to scheduling the biopsy. '"- PROVIDER SIGNATURE: ~ ~ ii.i DATE: Initiation of Treatment 0 Final eligibility determination completed. Liver biopsy results have been reviewed With the Regional Medical Director. 0 Provider reviews Schering.Plough Pegasys "Medication Guide" with th, patient ood provides education InterferonlRibavirin treatment. 0 Patient signs informed consent for InterferonfRibavirin treatment, a second time. 0 Provider completes Formulary Exception Request form and orders medication treatment. " PROVIDER SIGNATURE: 00 DATE: Safety and Efficacy Monitoring t- O Provider orders appropriate hematological and biochelPJcal testing and viral load testing as required on the HeV treatment ; flow sheet. The provider addresses compliance at each visit and asks specific questions for depression and suicidal ideation. PROVIDER SIGNATURE: DATE: ''"" Hev Program Evaluation Alabama Department of Corrections March 2004 Attachment E EVIDENCE OF COMPENSATED CIRRHOSIS Cirrhosis of the liver can be difficult to recognize ifit is still in the early stages where the body is able to compensate for those biochemical and circulatory changes, which when advanced, become obvious to the caregiver. Some physical findings related to more advanced cirrhosis that can be picked up easily are jaundice, ascites, asterixis, mental status changes, telangiectasias, and caput medusae. Certain laboratory studies can be helpful in diagnosing compensated cirrhosis. Tbese are albumin and prothrombin time, cac and platelets and LFrs including bilirubin. (Order a Diagnostic Profile 1 and Protime). Results of a complete blood count can point towards cirrhosis as well. Thrombocytopenia, leukopenia and anemia can result from hypersplenism secondary to the portal hypertension of cirrhosis. Thrombocytopenia is the most common abnonnality followed by leukopenia and then anemia. Neutropenia is the predominant finding related to leukopenia. Hypersplenism may result in any single abnonnality or any combination of abnonnalities. These low counts are caused by sequestration in the spleen. In the case of platelets, up to 90% of the total platelet mass can be found in the spleen. White cells and platelets seem to have approximately normal survival time in the spleen and in fact may be available if required in other areas of the body Serum albumin and prothrombin time are dependent upon the synthetic capabilities of the liver which would be compromised if enough of the liver tissue is affected by scarring. Findings consistent with cirrhosis would be those of hypoalbuminemia and elevated Il\iR. Findings of normal to low AST and ALT can also be seen in cirrhosis. In the case of chronic hepatitis C one might expect to find elevated liver enzymes but because of the presence of cirrhotic tissue the amount of functioning liver tissue is reduced. This limits the number ofnonnal hepatocytes that are able to leak enzymes that would nonnally result in the elevation of these serum levels. Additionally, it has been noted that in cirrhosis the ratio of AST to ALT can be greater than one. In chronic hepatitis C without cirrhosis this relationship is usually reversed. Hyperbilirubinemia can be found in cirrhosis. Usually elevated total and direct bilirubin will be found but elevated indirect bilirubin can be found at times. Clinically apparent jaundice is ordinarily not evident until bilirubin levels reach about 3 mgldl. Patients with compensated cirrhosis should have an AFP and liver ultrasound prior to starting treatment for Hep C to screen for HCC (hepatocellular carcinoma). Hypersplenism Sudeep K. Aulakh, M.D., F.R.C.P.c., Fern's Clinical Advisor 2003 Splenomegaly Lewis Kaplan, MD FACS, Department of Surgery, Division of Trauma and Critical Care, Yale University School of Medicine on emedicine 2003 Proposed Hepatitis C Prolocol Alabama Department of Corrections Page 1 March 2004 Attachmenl F HEPATITIS C TREATMENT FLOW SHEET 10 Number Patient Name Date of Birth __ First _~' Baseline 2 weeks 4 weeks 8 weeks 12 weeks I Facility '_~ 20 weeks 16 weeks 24 weeks I Date Vital Signs Blood Pressure Pulse Respirations Temperature Weight laboratory Studies HCV RNA Quantitative ' CBC w/dirr WBC~ Platelets~ Creatinine TSH 3 Pregnancy Test 2 0 NA HAV&HBV Dates(ir applicable) Mental Health Questions HAV #1 #2 HBV #1 .2 #3 2 C<lmpliance Counseling 2 Provider Signature o o Dale treatment Iniliate.d: Treatmenl discontinued due to: o Failed Response. 0 Patient initiated. 0 Contraindications. Date: _ _ ' _ _ ' _ _ (mm/ddfyfl Reason: _ Dale patient completed ther<lDV: , I (mm/dd/vvl o 1 Completed prior 10 initiation of themllY, at 12 weeks and 24 weeks following initiation of thewpy, upon completion and 6 months following the completion of therapy. !f there is not at least a 2-109 decrease In HCV RNA at 12 weeks, treatment will be discontinued. If HCV RNA still shows measurable virus at 24 weeks, treatment will be discontinued. 2 Completed al each scheduled chronic care visit. 3 To be completed every three months during therapy and 6 months post end of lfcatment. A copy 01 this form is to bo submitted to the R,,,ional Medical Director upon comptcUon or disoonUnuaUon of therapy. Hepatitis C Treatment Flow Sheet Alabama Department 01 Corrections Page 1 February 2003 Attachment G PEGLYATED INTERFERON AND RIBAVIRIN DOSAGE 1. Peglntron (Alfa 2B) • 1.5 mcglKglweek I. Pegasys (Alfa 2A) • 180 mcg weekly 2. Ribavirin • (400mg BID dosing) (DOT) • 800 mg daily. genotype - 2 & 3 • genotype la & 1b - >75 Kilo 41200 mg daily 2. Ribavirin • (400 mg BID dosing) (DOT) • 800 mg daily - genotype· 2 & 3 • genotype 4 - <75 Kilo - 1000 mg daily • genotype 1a & Ib - >75 Kilo - 1200 mg daily • genotype 4 -<75 Kilo ·1000 mgdaily • genotype 4 - >75 Kilo - 1200 mg daily Ribavirin Dosage Modification Guidelines Laboratory Values Hemoglobin in patients with no cardiac disease Hemoglobin in patients with history of stable cardiac disease Reduce Only Ribavirin Dose to 600 mcr/dav if: < 10 gldL Discontinue Ribavirin if: :S 2 g1dL decrease in hemoglobin < 12 g1dL despite 4 weeks at reduced dose during any 4 week period treatment < 8.5 gldL Hematological Hematological Dose Modification Guidelines Laboratory Values ANC <1000/mrn' Platelet <1 OO,OOO/nun Pel!3SYS Dose Reduction 135 ~g 90 "g Discontinue Pel!3SVS if: J ANC <500/mm , treatment should be suspended until ANe values return to more than I OOO/mm3• Reinstitute at 90 j..tg and monitor ANC. Platelet count <25,OOO/mm . Renal In patients with end-stage renal disease requiring Renal Dialysis, dose reduction to 135 mcg of Pegasys is recommended. Patients with a creatine clearance of less than 50 cc/minute, Pegasys should not be used. Proposed Hepatitis C Protocol - Alabama Depanment of Corrections Page 1 of2 December 31, 2003 Dose Modification - Pegasvs Gener-al When dose modification is required for moderate or severe adverse reactions, initial dose reduction to 135 meg (0.75 ml) is generally adequate_ However, in some cases, dose reduction to 90 meg (0.5 ml) may be needed. Following improvement of the adverse reaction, re-escalation of the dose may be considered. Guidelines for Dose Modification and Discontinuation of PEG-Iotron or PEG InterferonlRibavirin for Hematologic Toxicity Laboratory Values Hgb* WBC Neutrophil Platelets • PEG-Intron <1O.Ogldl <8.5.1dl <1.5 xlO /L <1.0 xl0 9/L <0.75 xlO IL <0.5 x 10'IL <80 xlO'IL <50 xlO'lL Permanently discontinue Reduce dose by 50% Pennanentlv discontinue Reduce dose by 50% Permanently discontinue Reduce dose by 50% Permanently discontinue Rebetol Decrease by 200mglday Pennanentlv discontinue Pennanentlv discontinue . ---"---. . .. Pennanently discontinue _ -- ----- _. .--. . - ------.- Permanently discontinue For patients wilh a history of stable cardiac disease receiving PEG-Intron in combination Ribavirin, the PEG-Intron dose should be reduced by half and the Ribavirin dose by 200mglday if a> 2g1dL decrease in hemoglobin is observed during any 4 week period. Both PEG-Intron and Ribavirin should be pennanently discontinued ifpatients have hemoglobin level < than 12 gldL after this Ribavirin dose reduction. Recommended dose of Ribavirin (BID dosing) (given via DOT) < 65 Kilo - 800mg daily > 65 - 85 Kilo - I OOOmg daily > 85 Kilo - 1200rng daily Genotype-non IA & IB 800mg daily Proposed Hepatitis C Protocol- Alabama Depanment ofCorrectiof'.s Page 2 of2 December 31, 2003 Attaclunent H CLINICAL GUIDELI IES FOR EVALUATION OF ALPHA FETO PROTEIN AJ'ID HEPTOCELLULAR CARCINOMA (HCC) ./ After birth serum levels fall to ihe normal (below 20 ng/ml). ./ Modest elevations (greater than 20) but seldom greater than 400 can occur in acute or chronic liver injury. ./ In cirrhotic patients, a steady increase or levels greater than 500 nglml are indicative of HCC. ./ Levels of 500 nglml indicate tumor size of2·3 cm. ./ Levels tend to stabilize in individual patients regardless of rumor size. ./ AFP done rou[inely on all cirrhosis patients - monitor every six months. ./ ASTIALT ratio - yearly. Proposed Hepatitis C PrOlocol - Alab::mla. Departm=nt of Corrections Page I March 2004 Attachment I Interferon - Ribavirin Side Effects Symptoms Prevention and Management Fever, chills, and muscle and joint pains are frequently encountered with the start of interferon/ribavirin therapy. Symptoms generally begin between 2·12 hours after injection. The worst symptoms may occur during the first 3 injections, usually subside in severity within 1-2 months of therapy, but persist to some degree during the course of treatment. By administering the injections as late in the day as possible, the individual may sleep through the worst symptoms. Encouraging adequate fluid intake and rest may reduce symptom severity. Pre-treatment with the medications listed below can significantly reduce these side effects. Acetaminophen, 500 mg tabs, 2 tablets with each Interferon injection. May repeat up to three times daily to reduce or relieve flu-like symptoms. OR Ibuprofen, 200 mg tabs, 2 tablets with each Interferon injection. May repeat up to three times daily to reduce or relieve flu-like symptoms. Headache frequently accompanies other "flu-like" symptoms associated with Interferon injections. It is important to rule out other conditions. Assess neurological status, look for other causes: hydration status, migraine history, HTN, dental problems, allergies, other drug interactions, stress, sleep disturbances, honnanal changes, caffeine, anemia, need for new glasses. Therapy should be supportive in nature and address problems that can be corrected, such as limiting light and sound stimulation. Consider the use ofNSAIDS, Fioricet, acetaminophen, or amitriptyline therapy. Myalgia/neuralgia also frequently accompanies other "flu-like" symptoms associated with interferon injections. Encourage mild, low impact exercise and wann compresses to affected areas. Fatigue is often associated with interferon injections and often persists to some degree throughout the course of therapy. These symptoms can be minimized by maintaining hydration, encouraging moderate exercise, energy conservation and maintaining good nutrition. Nausea, vomiting and/or diarrhea can result from interferonlribavirin therapy. Symptoms can become so severe that maintaining weight and nutritional status becomes a big challenge. Effects may be managed by encouraging frequent small meals, avoidance of acidic, spicy or greasy foods and providing nutritional supplements. Monitor electrolytes as needed. Anti-emetics and anti-diarrhea agents may need to be used. Taste alterations specifically, complaint of metallic taste in the mouth is common with therapy. This can add to the anorexia experienced by patients during therapy. Advising the use of plastic utensils, drinking cranberry juice or lemonade and using hard candy mints, chocolate and citrus drinks may lessen severity. Alopecia usually presents as a slow progression in severity over the course of therapy and is reversible with discontinuation of treatment. Encourage measures to diminish severity such as the use of mild HCV Program - Alabama Department of Corrections Side Effects Page10f2 March 2004 shampoos and conditioners. constrictive head wear. Stress avoidance of hair products that cause dryness and wearing Cough may develop during therapy. Assess pulmonary status with PFT or CXR as indicated, rule out other causes such as allergies or asthma SuppoItive therapies include increased fluid intake, use of a humidifier. avoidance of irritants such as smoke and aerosol sprays, and sucking on hard candy or cough drops. Itching and rash can occur. Assess baseline skin condition; consider autoimmune conditions such as psoriasis. Monitor liver and renal functions tests. Symptoms can be minimized by encouraging use of mild soaps and wearing sunscreen when outside. If symptoms persist, consider ore hydrocortisone cream and antihistamines. Mood Disturbances, namely depression, anxiety, initability and insomnia are common. interferon/ribavirin therapy tends to worsen pre-existing symptoms, and these problems need to be addressed and stabilized prior to beginning therapy. "SEVERE PSYCHIATRIC EVENTS HAVE OCCURRED WITH INTERFERON THERAPIES, INCLUDING DEPRESSION, PSYCHOSES, AGGRESSIVE BEHAVIOR, HALLUCINATIONS, VIOLENT BEHAVIOR, HOMICIDAL IDEATION, SU/DICAL IDEATION, ATTEMPTS AND SUICIDES IN PATIENTS WITH AND fVITHOUT PREVIOUS PSYCHIATRIFC DISORDERS" Hematology Concerns Ribavirin Induced Hemolytic Anemia: Hemoglobin levels generally decrease from baseline within the first 4 weeks of combination therapy. A mean decrease between 2-3 gldL is common. Hemoglobin levels usually stabilize after 4 weeks of therapy and return to pretreatment levels within 8 weeks of discontinuation. As levels decline, patients often complain of shortness of breath with any exertion, chest pain, weakness, fatigue and anorexia. People with pre-existing cardiovascular disease must be closely monitored. Dose reduction of ribavirin according to modification guidelines may be necessary and education and reassurance is important in preventing early tennination. Neutropenia commonly occurs with interferon therapy, is transient in nature and usually occurs within the first few weeks of initiation of therapy. It often lasts for the duration of therapy and recovery to baseline levels occurs upon cessation of treatment. Monitor labs according to protocol, and management involves dose reduction of interferon when ANC levels fall <7S0/rnrn J • Thrombocytopenia may be sudden and severe enough to discontinue therapy. Watch platelet counts carefully, and refer to dose reduction table if platelets drop below SO,OOO/mm . Advise patients to report bruising, nosebleeds or petechiae. HCV Program - Alabama Department of Corrections Side Effects Page 2 of 2 March 2004 Attachment J Summary National Institutes of Health Consensus Development Conference Statement Management of Hepatitis C Final Statement *The complete 44-page document can be found at http://vvww.nih.gov/. The NIH Consensus Development Conference on Management of Hepatitis C: 2002 was held June 10 - 12, 2002. The final statement was published September 12, 2002. The "Final Statement" contains the following disclaimers: 1. "This statement is not a policy statement of the NIH or the Federal Government" and 2. "Thus, it provides a "snapshot in time" of the state of knowledge". The Virus The lack of a vigorous T-lymphocyte response and the high propensity of the virus to mutate appear to promote a high rate of chronic infection. The extensive genetic heterogeneity of Hepatitis C virus (HCY) has important diagnostic and clinical implications, perhaps explaining difficulties in vaccine development and the lack of response to therapy. Genotype 1 accounts for 70 to 75 percent of all HeV infections in the United States and is associated with a lower rate of response to treatment. Hey replicates preferentially in hepatocytes but is not directly cytopathic. DUrin~ chronic infection, HeV RNA reaches high levels, generally ranging from 105 to 10 international units (W)/mL, but the levels can fluctuate widely. However, within the same individual, RNA levels are usually relatively stable. Epidemiology Although difficult to assess accurately, the incidence of ReV infections declined sharply in the late 19805. However, the estimated prevalence of HeV in the U.S. is at least 1.8 percent of the population and a fourfold increase in the number of adults diagnosed with chronic HCV infection is projected from 1990 to 2015. Currently, persons aged 40 to 59 years have the highest prevalence ofHCV infection, and in this age group, the prevalence is highest in African Americans (6.1%). High HCV seroprevalence rates (from 15-50 percent) have occurred in specific subpopulation, such as homeless, incarcerated persons, injection drug users, and persons with hemophilia who were treated with clotting factors before 1992. The highest seroprevalence rates (70 to more than 90 percent) have been reported in the last of these two groups Chronic Infection Hepatitis C Position Statement - Alabama Department of Corrections Summary ofNrH Statement Page I 0£8 February, 2003 Persistence ofHCV infection is diagnosed by the detection ofHCV RNA in the blood for at least 6 months. In general, prospective studies have shown that 60 to 85 percent of HCV-infected persons develop chronic infection. The most important sequelae of chronic HCV infection are progressive liver fibrosis leading to cirrhosis, end·stage liver disease, and Hepatocellular Carcinoma (HCC). Estimates of the proportion of chronically infected persons who develop cirrhosis 20 years after initial infection vary widely from 2 to 4 percent in studies of children and young women to as high as 20 to 30 percent in middle-aged transfused subjects. The actual risk is likely intermediate between these two ranges, on the order of 10 to 15 percent. There is little evidence that virologic factors, including viral load, viral genotype. and quasi-species diversity significantly affect the risk of progression of liver disease. However, many host factors increase this risk, including: » » » » » » Older age at time of infection, Male gender, Immunosuppression such as that associated with HIV infection, and Concurrent chronic hepatitis B infection. Higher levels of alcohol use play an important role in promoting the development of progressive liver disease, with strong evidence for the detrimental effects of 30 glday in men (- equivalent to 2 beers, 2 glasses of wine, or 2 mixed drinks) and 20 glday in women. Conversely, individuals infected at a younger age have little or no disease progression over several decades. Hepatocellular Carcinoma Hec rarely occurs in the absence of cirrhosis or advanced fibrosis. Risk factors for HCC in persons with chronic HeV infection are largely the same as those for the development of decompensated cirrhosis. Some but not all studies suggest that treatment with interferon and ribavirin may reduce the risk of developing HCC in HCV patients with cirrhosis, but more data are needed. Hev Serologic Assays Enzyme immunoassay (ELI\.) tests are reproducible, inexpensive, and FDA·approved for use in the diagnosis of HCV infection. The very high sensitivity (low rate of false negative) and specificity (low rate of false positive) of the version 3 (third-generation) EIAs (sensitivity of greater than 99 percent, specificity of 99 percent in immunocompetent patients) obviate the need for a confirmatory immunoblot assay in the diagnosis of individual patients with clinical liver disease, particularly those with risk factors for HCV infection. Qualitative HCV RNA Assays Chronic HCV infection in a patient with a positive ElA test should be confirmed by a qualitative HCV RNA assay with a lower limit of detection of 50 IU/mL or less (approximately 100 viral genes/mL). A single positive qualitative assay for HCV RNA Hepatitis C Position Statement - Alabama Department of Corrections Sununary ofNlli Statement Page20f8 February, 2003 confirms active HeV replication, but a single negative assay does not exclude viremia and may reflect only a transient decline in viral level below the level of detection of the assay. Until future studies determine whether the sustained virological response (SVR) will be sustained over the long term following successful antiviral treatment, periodic measurements ofHCV RNA may need to be performed. Quantitative HeV RNA Assays Testing for HeV RNA level (or viral load) with a quantitative assay provides accurate information on HeV viral levels. Significant variability exists between available assays. The clinical utility of serial HCV viral levels in a patient is predicated on continued use of the same specific quantitative assay that was used in the initial determination of the viral level. While there is little correlation between disease severity or disease progression with the absolute level ofHCV RNA, quantitative determination of the HCV level provides important information on the likelihood of response to treatment in patients undergoing antiviral therapy. ALT Testing for serum ALT levels is the most inexpensive and noninvasive, but relatively insensitive, means of assessing disease activity. Serial determinations of ALT levels over time may provide a better means of assessing liver injury, but the accuracy of this approach has not been well documented. Patients who initially have a nonnal ALT level should undergo serial measurements over several months to confinn the persistence of normal ALT levels. Although loss or reduction in HCV RNA is the primary indicator of response to antiviral therapy, the resolution of elevated ALT levels with antiviral therapy appears to be an important indicator of disease response. Noninvasive Tests of Fibrosis No single test or panel of serologic markers can provide an accurate assessment of intermediate stages of hepatic fibrosis. Similarly, quantitative tests of liver function and radiologic imaging of the liver are sensitive for diagnosing advanced cirrhosis but are not useful in assessing hepatic fibrosis and early cirrhosis. Liver Biopsy Liver biopsy provides a unique source of information on fibrosis and assessment of histology. The information obtained on liver biopsy allows affected individuals to make more infonned choices about the initiation or postponement of antiviral treatment. Thus, the liver biopsy is a useful part of the informed consent process. In general, a baseline assessment of liver histology offers a valuable standard for subsequent comparisons. However, the appropriate interval for subsequent evaluations is yet to be detennined. Hepatitis C Position Statement - Alabama Department of Corrections Surrunary ofNTI-I Statement Page 3 0[8 February, 2003 Liver biopsy can provide direct histologic assessment of liver injury due to HCV but cannot be used to diagnose HCV infection. Hepatocellular Carcinoma Screening HCC complicates cirrhosis secondary to HCV. It is estimated that HCC occurs after the development of cirrhosis at a rate varying from 0 to 3 percent per year. Alpha-fetoprotein (AFP) and ultrasound every 6 months were used in a single study of patients with cirrhosis secondary to HCV. Identification ofHCC was not significantly increased in the screened population. The value of screening for AFP is uncertain because there are no available data to demonstrate the clinical impact of this screening on the management of HCC or associated mortality. Studies of the performance characteristics of AFP and hepatic ultrasound show that AFP has a poor sensitivity and a high rate of false-positive reactions. Hepatic ultrasound is more sensitive than AFP testing but is also more expensive, and it can lead to invasive and unnecessary evaluations of lesions (e.g., regenerative nodules, hemangiomas, hepatic cysts) that are not HCc. However, such routine AFP or imaging screening should not be performed in patients with HCV in the absence of cirrhosis because HCC is so rare in this group. What is the most effective therapy for hepatitis C? Currently the best indicator of effective treatment is an SVR, defined by the absence of detectable HCV RNA in the serum as shown by a qualitative HCV RNA assay with lower limit of detection of 50 IU/mL or less at 24 weeks after the end oftreatment. Treatment of Naive Patients Three large pivotal trials have examined the efficacy of pegylated interferon plus ribavirin in the treatment of chronic HCV infection. Overall, pegylated interferon plus ribavirin was more effective than standard interferon-ribavirin combination or pegylated interferon alone. Among patients with genotypes 2 or 3, SVRs with standard interferon and ribavirin were comparable to those with pegylated interferon and ribavirin, and thus standard interferon and ribavirin could be used in treating patients with these genotypes. In a recent study, a 24-week course of pegylated interferon and ribavirin was found to be as effective as a 48-week course in patients with genotypes 2 and 3 (SVR rates of 73 to 78 percent), but not in patients with genotype 1 (SVR rates of 41% with 24 weeks and 51% with 48 weeks). Similarly, a reduced ribavirin dosage of 800 mg daily appeared to be adequate for patients with genotypes 2 and 3, but the higher, standard dosage of 1000 to 1200 mg daily yielded better response rates in patients with genotype 1. Thus, 24 weeks of treatment and an 800 mg dose of ribavirin appear to be sufficient for persons with genotypes 2 and 3, while patients with genotype 1 need 48 weeks of treatment and standard doses of ribavirin. Early viral response (EVR) defined, as a minimum 2-log decrease in viral load during the first 12 weeks of treatment, is predictive of SVR and should be a routine part of monitoring patients with genotype 1. Patients who fail to achieve an EVR at week 12 of treatment have only a small chance of achieving an SVR even if therapy is continued for Hepatitis C Position Statement - Alabama Department of Corrections Summary ofNIH Statement Page 4 of 8 February, 2003 a full year. Treatment need not be extended beyond 12 weeks in these patients. Although an SVR is difficult to correlate with improved survival because ofthe necessity for longterm follow-up, the absence of detectable serum HCV RNA has been associated with resolution of liver injury, reduction in hepatic fibrosis, and a low likelihood of a relapse of the HCV infection. Additionally, in two large but uncontrolled long-term follow-up studies from Japan, SVR after interferon treatment was associated with a lower risk of BCe. Conversely, one observational Italian study with long-term follow-up found no difference in development ofHCC between those with and without interferon treatment. Re-treatment of Patients Studies are currently being conducted with pegylated interferon and ribavirin therapy in patients who relapsed after interferon monotherapy or standard interferon and ribavirin therapy. Failure to respond to optimal therapy with pegylated interferon and ribavirin presents a significant problem, particularly in the presence of advanced fibrosis or cirrhosis. Currently, several large-scale, multicenter u.s. trials are evaluating the role of maintenance therapy with pegylated interferon alone in preventing further progression of cirrhosis, clinical decompensation, or development of HCe. Until the results of these studies are available, the role of long-term, continuous therapy with pegylated interferon (or ribavirin or both) for nonresponders should be considered experimental. Adherence Patient adherence is critical to the success of treatment of HCV.Physicians should discuss the importance of adherence with patients before embarking on therapy and regularly assess and take steps to help their patients maximize their adherence. Such measures include management of side effects, depression, and substance abuse. Side Effects of Treatment In registration trials of pegylated interferon and ribavirin, significant side effects resulted in discontinuation of treatment in approximately 10 to 14 percent of patients. Major side effects of combination therapy include influenza-like symptoms, hematologic abnormalities, and neuropsychiatric symptoms. The education of patients, their family members, and caregivers about side effects and their prospective management is an integral aspect of treatment. Frequent monitoring of neuropsychiatric side effects, cytopenia, and adherence to HCV therapy is necessary. Psychological conditions, particularly depression, are common among persons with HCV and are frequent side effects of interferon. The patient's mental health status should be assessed before beginning antiviral therapy and monitored regularly during therapy. It is not known if the use of hematopoietic growth factors will enhance the likelihood of SVR. Thus, the benefits of such treatment need to be proven prospectively before it can be recommended. Hepatitis C Position Statement - Alabama Department of Corrections Summary of NIB Statement Page 5 of 8 February, 2003 Which patients with hepatitis C should be treated? All patients with chronic HCV are potential candidates for antiviral therapy. Treatment is recommended for patients with an increased risk of developing cirrhosis. These patients are characterized by: >- Detectable HCV RNA levels higher than 50 IU/mL, >- A liver biopsy with findings of portal or bridging fibrosis, and at least Moderate inflammation and necrosis, and >- Persistently elevated ALT values. Because a large number of HCV-infected persons in the United States are incarcerated, programs should be implemented to prevent, diagnose, and treat HCV infection in these individuals. Patients with chronic HCV should be vaccinated against hepatitis A, and seronegative persons with risk factors for hepatitis B virus (HBV) should be vaccinated against HBV. Normal ALT Levels Approximately 30 percent of patients with chronic HCV infection have normal ALT levels, and another 40 percent have ALT levels less than two times the upper limit of normal (70% have <2x the upper limit). Although most of these patients have mild disease, histologically, some may progress to advanced fibrosis and cirrhosis. Experts differ on whether to biopsy and treat these patients. Studies of pegylated interferon with ribavirin have not been completed in patients with normal ALT levels. Mild Liver Disease Progression to cirrhosis is likely to be slow in patients who have persistent ALT elevations but no fibrosis and minimal necroinflammatory changes. These patients may not need treatment and should be monitored periodically. Recurrence After Transplantation Hepatitis C frequently recurs following liver transplantation, and disease progression is accelerated compared with immunocompetent patients with HCV disease. Once cirrhosis develops in the allograft, the risk of complications is high. While recurrence of HCV replication is almost universal after liver transplantation, the severity of the recurrence of HCV after transplant correlates with the degree of immunosuppression in the posttransplantation period. Treatment of HCV recurrence after liver transplantation should be considered experimental and carried out in the context of clinical trials. Hepatitis C Position Statement - Alabama Department of Corrections Summary ofNIH Statement -- -- Page 6 of 8 February, 2003 Active Injection Drug Users Recent, albeit limited, experience has demonstrated the feasibility and effectiveness of treating chronic HCV in people who use illicit injection drugs, known as injection drug users (IDUs). Treatment for drug and alcohol abuse should be made available to all patients who want and need it. However, few data are available on HCV treatment in active IDUs who are not in drug treatment programs. Thus, it is recommended that treatment of active injection drug use be considered on a case-by-case basis, and that active injection drug use in and of itself not be used to exclude such patients from antiviral therapy. HIV Co-infection Although there are no HCV therapies specifically approved for patients co-infected with HIV, these patients should be considered for treatment. Alcohol and HCV Alcohol is an important cofactor in the progression of HCV liver disease to cirrhosis and HCC. A history of alcohol abuse is not a contraindication to therapy; however, continued alcohol use during therapy adversely affects response to treatment, and alcohol abstinence is strongly recommended before and during antiviral therapy. Heavy alcohol consumption of >80 g/day seriously compromises HCV treatment. Furthermore, safe levels of alcohol consumption are still unclear, and even moderate levels of consumption may accelerate disease progression in some patients. Recommendations to be made to patients to prevent transmission of hepatitis C The large reservoir of individuals infected with HCV provides a source of transmission to others at risk. Direct percutaneous exposure is the most efficient method for transmitting HCV, and injection drug use accounts for more than two-thirds of all new infections in the United States. Methadone treatment programs, needle and syringe exchange programs, and comprehensive risk-modifying educational programs have been shown to be effective in preventing HIV transmission and are likely to be useful for decreasing HCV transmission. Ensuring access to sterile syringes through physician prescription and pharmacy sales of syringes to IDUs can also be helpful. IDUs should be educated about the importance of hand washing before and after giving injections, not using the others' injection equipment, and avoiding any contact with blood from other persons. HCV prevention education should be a high priority in correctional settings. In the United States, the estimated seroprevalence of HCV is 2 to 3 percent among partners of HCV-infected persons who are in long-term monogamous relationships and is 4 to 6 percent among persons with multiple sex partners, sex workers, and men who have sex with men (those at risk for sexually transmitted diseases). One study found the risk of HCV infection to be threefold higher for female than male sexual partners. Because of the low risk of HCV transmission, monogamous couples do not need to use barrier protection (condoms) although they should be advised that condoms may reduce the risk of transmission. There is no evidence that kissing, hugging, sneezing, coughing, food, Hepatitis C Position Statement - Alabama Department of Corrections Summary ofNIH Statement Page 7 of 8 February, 2003 water, sharing eating utensils or drinking glasses, casual contact, or other contact without exposure to blood is associated with HCV transmission for correctional staff. Body piercing and tattooing are other potential sources of transmission if contaminated equipment or supplies are used. However, transmission through these activities is rare and confounded by other risk factors. RECOMMENDATIONS ~ Educate the American public on the transmission of HCV in order to better identify affected individuals and to institute preventive measures. ~ Promote the establishment of screening tests for all groups at high risk of HCV infection, including mus and incarcerated individuals. ~ Institute measures to reduce transmission of HCV among mus, including providing access to sterile syringes through needle exchange, physician prescription, and pharmacy sales; and expanding the Nation's capacity to provide treatment for substance abuse. Physicians and pharmacists should be educated to recognize that providing mus with access to sterile syringes and education in safe injection practices may be lifesaving. ~ Encourage a comprehensive approach to promote the collaboration among health professionals concerned with management of addiction. Primary care physicians, and specialists should be involved in various aspects of HCV management - to deal with the complex societal, medical, and psychiatric issues of mus afflicted by the disease. AttachmentJ Summary National Institutes of Health Consensus Development Conference Statement Management of Hepatitis C Final Statement *The complete 44-page document can be found at http://www.nih.gov/. The NIH Consensus Development Conference on Management of Hepatitis C: 2002 was held June 10 -12,2002. The final statement was published September 12, 2002. The "Final Statement" contains the following disclaimers: 1. "This statement is not a policy statement of the Nlli or the Federal Government" and 2. "Thus, it provides a "snapshot in time" of the state of knowledge". The Virus The lack of a vigorous T-Iymphocyte response and the high propensity of the virus to mutate appear to promote a high rate of chronic infection. The extensive genetic heterogeneity of Hepatitis C virus (HCY) has important diagnostic and clinical implications, perhaps explaining difficulties in vaccine development and the lack of response to therapy. Genotype 1 accounts for 70 to 75 percent of all HCY infections in _Jhe United States and is associated with a lower rate ofresponse to treatment. HCY replicates preferentially in hepatocytes but is not directly cytopathic. During chronic infection, HCV RNA reaches high levels, generally ranging from 105 to 107 international units (IU)/mL, but the levels can fluctuate widely. However, within the same individual, RNA levels are usually relatively stable. Epidemiology Although difficult to assess accurately, the incidence ofllCY infections declined sharply in the late 1980s. However, the estimated prevalence of HCY in the US. is at least 1.8 percent of the population and a fourfold increase in the number of adults diagnosed with chronic HCY infection is projected from 1990 to 2015. Currently, persons aged 40 to 59 years have the highest prevalence of HCY infection, and in this age group, the prevalence is highest in African Americans (6.1%). High HCV seroprevalence rates (from 15-50 percent) have occurred in specific subpopulation, such as homeless, incarcerated persons, injection drug users, and persons with hemophilia who were treated with clotting factors before 1992. The highest seroprevalence rates (70 to more than 90 percent) have been reported in the last of these two groups Chronic Infection Hepatitis C Position Statement Summary ofNlli Statement ,-- - Alabama Department of Corrections Page 1 of 8 February, 2003 Persistence ofHCV infection is diagnosed by the detection ofHCV RNA in the blood for at least 6 months. In general, prospective studies have shown that 60 to 85 percent of HCV-infected persons develop chronic infection. The most important sequelae of chronic HCY infection are progressive liver fibrosis leading to cirrhosis, end-stage liver disease, and Hepatocellular Carcinoma (HCC). Estimates of the proportion of chronically infected persons who develop cirrhosis 20 years after initial infection vary widely from 2 to 4 percent in studies of children and young women to as high as 20 to 30 percent in middle-aged transfused subjects. The actual risk is likely intermediate between these two ranges, on the order of 10 to 15 percent. There is little evidence that virologic factors, including viral load, viral genotype, and quasi-species diversity significantly affect the risk of progression of liver disease. However, many host factors increase this risk, including: ~ ~ ~ >>- Older age at time of infection, Male gender, Immunosuppression such as that associated with HIV infection, and Concurrent chronic hepatitis B infection. Higher levels of alcohol use play an important role in promoting the development of progressive liver disease, with strong evidence for the detrimental effects of 30 glday in men (~equivalent to 2 beers, 2 glasses of wine, or 2 mixed drinks) and 20 g/day in women. >- Conversely, individuals infected at a younger age have little or no disease progression over several decades. Hepatocellular Carcinoma HCC rarely occurs in the absence of cirrhosis or advanced fibrosis. Risk factors for HCC in persons with chronic HCV infection are largely the same as those for the development of decompensated cirrhosis. Some but not all studies suggest that treatment with interferon and ribavirin may reduce the risk of developing HCC in HCV patients with cirrhosis, but more data are needed. HCY Serologic Assays Enzyme immunoassay (ErA) tests are reproducible, inexpensive, and FDA-approved for use in the diagnosis of HCV infection. The very high sensitivity (low rate of false negative) and specificity (low rate of false positive) of the version 3 (third-generation) BIAs (sensitivity of greater than 99 percent, specificity of 99 percent in immunocompetent patients) obviate the need for a confirmatory immunoblot assay in the diagnosis of individual patients with clinical liver disease, particularly those with risk factors for HCV infection. Qualitative HCY RNA Assays Chronic HCV infection in a patient with a positive EIA test should be confirmed by a qualitative HCV RNA assay with a lower limit of detection of 50 IU/mL or less (approximately 100 viral genes/mL). A single positive qualitative assay for HCV RNA Hepatitis C Position Statement - Alabama Department of Corrections Summary ofNIH Statement Ii Page 2 of 8 February, 2003 confirms active HCV replication, but a single negative assay does not exclude viremia and may reflect only a transient decline in viral level below the level of detection of the assay. Until future studies determine whether the sustained virological response (SVR) will be sustained over the long term following successful antiviral treatment, periodic measurements of HCV RNA may need to be performed. Quantitative HCV RNA Assays Testing for HCV RNA level (or viral load) with a quantitative assay provides accurate information on HCV viral levels. Significant variability exists between available assays. The clinical utility of serial HCV viral levels in a patient is predicated on continued use of the same specific quantitative assay that was used in the initial determination of the viral level. While there is little correlation between disease severity or disease progression with the absolute level of HCV RNA, quantitative determination of the HCY level provides important information on the likelihood of response to treatment in patients undergoing antiviral therapy. ALT Testing for serum ALT levels is the most inexpensive and noninvasive, but relatively insensitive, means of assessing disease activity. Serial determinations of ALT levels over time may provide a better means of assessing liver injury, but the accuracy of this approach has not been well documented. Patients who initially have a normal ALT level should undergo serial measurements over several months to confirm the persistence of normal ALT levels. Although loss or reduction in HCV RNA is the primary indicator of response to antiviral therapy, the resolution of elevated ALT levels with antiviral therapy appears to be an important indicator of disease response. Noninvasive Tests of Fibrosis No single test or panel of serologic markers can provide an accurate assessment of intermediate stages of hepatic fibrosis. Similarly, quantitative tests of liver function and radiologic imaging of the liver are sensitive for diagnosing advanced cirrhosis but are not useful in assessing hepatic fibrosis and early cirrhosis. Liver Biopsy Liver biopsy provides a unique source of information on fibrosis and assessment of histology. The information obtained on liver biopsy allows affected individuals to make more informed choices about the initiation or postponement of antiviral treatment. Thus, the liver biopsy is a useful part of the informed consent process. In general, a baseline assessment of liver histology offers a valuable standard for subsequent comparisons. However, the appropriate interval for subsequent evaluations is yet to be determined. Hepatitis C Position Statement - Alabama Department of Corrections Summary ofNIH Statement Page 3 of 8 February, 2003 Liver biopsy can provide direct histologic assessment of liver injury due to HCV but cannot be used to diagnose HCV infection. Hepatocellular Carcinoma Screening HCC complicates cirrhosis secondary to HCV. It is estimated that HCC occurs after the development of cirrhosis at a rate varying ITom0 to 3 percent per year. Alpha-fetoprotein (AFP) and ultrasound every 6 months were used in a single study of patients with cirrhosis secondary to HCV. Identification of HCC was not significantly increased in the screened population. The value of screening for AFP is uncertain because there are no available data to demonstrate the clinical impact of this screening on the management of HCC or associated mortality. Studies of the performance characteristics of AFP and hepatic ultrasound show that AFP has a poor sensitivity and a high rate of false-positive reactions. Hepatic ultrasound is more sensitive than AFP testing but is also more expensive, and it can lead to invasive and unnecessary evaluations of lesions (e.g., regenerative nodules, hemangiomas, hepatic cysts) that are not HCc. However, such routine AFP or imaging screening should not be performed in patients with HCV in the absence of cirrhosis because HCC is so rare in this group. What is the most effective therapy for hepatitis C? Currently the best indicator of effective treatment is an SVR, defined by the absence of detectable HCV RNA in the serum as shown by a qualitative HCV RNA assay with lower limit of detection of 50 IU/mL or less at 24 weeks after the end oftreatment. Treatment of Naive Patients Three large pivotal trials have examined the efficacy of pegylated interferon plus ribavirin in the treatment of chronic HCV infection. Overall, pegylated interferon plus ribavirin was more effective than standard interferon-ribavirin combination or pegylated interferon alone. Among patients with genotypes 2 or 3, SVRs with standard interferon and ribavirin were comparable to those with pegylated interferon and ribavirin, and thus standard interferon and ribavirin could be used in treating patients with these genotypes. In a recent study, a 24-week course ofpegylated interferon and ribavirin was found to be as effective as a 48-week course in patients with genotypes 2 and 3 (SVR rates of 73 to 78 percent), but not in patients with genotype 1 (SVR rates of 41% with 24 weeks and 51% with 48 weeks). Similarly, a reduced ribavirin dosage of 800 mg daily appeared to be adequate for patients with genotypes 2 and 3, but the higher, standard dosage of 1000 to 1200 mg daily yielded better response rates in patients with genotype 1. Thus, 24 weeks of treatment and an 800 mg dose of ribavirin appear to be sufficient for persons with genotypes 2 and 3, while patients with genotype 1 need 48 weeks of treatment and standard doses ofribavirin. Early viral response (EVR) defined, as a minimum 2-log decrease in viral load during the first 12 weeks of treatment, is predictive of SVR and should be a routine part of monitoring patients with genotype 1. Patients who fail to achieve an EVR at week 12 of treatment have only a small chance of achieving an SVR even if therapy is continued for Hepatitis C Position Statement - Alabama Department of Corrections Summary ofNIH Statement IIiII Page 4 of 8 February, 2003 a full year. Treatment need not be extended beyond 12 weeks in these patients. Although an SVR is difficult to correlate with improved survival because of the necessity for longterm follow-up, the absence of detectable serum HCV RNA has been associated with resolution of liver injury, reduction in hepatic fibrosis, and a low likelihood of a relapse of the HCV infection. Additionally, in two large but uncontrolled long-term follow-up studies ITom Japan, SVR after interferon treatment was associated with a lower risk of HCC. Conversely, one observational Italian study with long-term follow-up found no difference in development ofHCC between those with and without interferon treatment. Re-treatment of Patients Studies are currently being conducted with pegylated interferon and ribavirin therapy in patients who relapsed after interferon monotherapy or standard interferon and ribavirin therapy. Failure to respond to optimal therapy with pegylated interferon and ribavirin presents a significant problem, particularly in the presence of advanced fibrosis or cirrhosis. Currently, several large-scale, multicenter u.S. trials are evaluating the role of maintenance therapy with pegylated interferon alone in preventing further progression of cirrhosis, clinical decompensation, or development of HCc. Until the results of these studies are available, the role of long-term, continuous therapy with pegylated interferon (or ribavirin or both) for nonresponders should be considered experimental. Adherence Patient adherence is critical to the success of treatment of HCV. Physicians should discuss the importance of adherence with patients before embarking on therapy and regularly assess and take steps to help their patients maximize their adherence. Such measures include management of side effects, depression, and substance abuse. Side Effects of Treatment In registration trials of pegylated interferon and ribavirin, significant side effects resulted in discontinuation of treatment in approximately 10 to 14 percent of patients. Major side effects of combination therapy include influenza-like s)'l11ptoms, hematologic abnormalities, and neuropsychiatric symptoms. The education of patients, their family members, and caregivers about side effects and their prospective management is an integral aspect of treatment. Frequent monitoring of neuropsychiatric side effects, cytopenia, and adherence to HCV therapy is necessary. Psychological conditions, particularly depression, are common among persons with HCV and are frequent side effects of interferon. The patient's mental health status should be assessed before beginning antiviral therapy and monitored regularly during therapy. It is not known if the use of hematopoietic growth factors will enhance the likelihood of SVR. Thus, the 1:>enefitsof such treatment need to be proven prospectively before it can be recommended. Hepatitis C Position Statement - Alabama Department of Corrections Summary ofNIH Statement Page 5 of 8 February, 2003 ---~ Which patients with hepatitis C should be treated? All patients with chronic HCV are potential candidates for antiviral therapy. Treatment is recommended for patients with an increased risk of developing cirrhosis. These patients are characterized by: » DetectableHCVRNA levelshigherthan 50 IU/mL, » A liver biopsy with findings of portal or bridging fibrosis, and at least Moderate inflammationand necrosis, and » PersistentlyelevatedALT values. Because a large number of HCV-infected persons in the United States are incarcerated, programs should be implemented to prevent, diagnose, and treat HCV infection in these individuals. Patients with chronic HCV should be vaccinated against hepatitis A, and seronegative persons with risk factors for hepatitis B virus (HBV) should be vaccinated against HBV. Normal ALT Levels Approximately 30 percent of patients with chronic HCV infection have normal ALT levels, and another 40 percent have ALT levels less than two times the upper limit of normal (70% have <2x the upper limit). Although most of these patients have mild disease, histologically, some may progress to advanced fibrosis and cirrhosis. Experts differ on whether to biopsy and treat these patients. Studies of pegylatedinterferon with ribavirin have not been completed in patients witfi~ normal ALT levels. Mild Liver Disease Progression to cirrhosis is likely to be slow in patients who have persistent ALT elevations but no fibrosis and minimal necroinflammatory changes. These patients may not need treatment and should be monitored periodically. Recurrence After Transplantation Hepatitis C fTequently recurs following liver transplantation, and disease progression is accelerated compared with immunocompetent patients with HCV disease. Once cirrhosis develops in the allograft, the risk of complications is high. While recurrence of HCV replication is almost universal after liver transplantation, the severity of the recurrence of HCV after transplant correlates with the degree of immunosuppression in the posttransplantation period. Treatment of HCV recurrence after liver transplantation should be considered experimental and carried out in the context of clinical trials. Hepatitis C Position Statement - Alabama Department of Corrections Summary ofNIH Statement Page 6 of 8 February, 2003 Active Injection Drug Users Recent, albeit limited, experience has demonstrated the feasibility and effectiveness of treating chronic HCV in people who use illicit injection drugs, known as injection drug users (IDUs). Treatment for drug and alcohol abuse should be made available to all patients who want and need it. However, few data are available on HCV treatment in active IDUs who are not in drug treatment programs. Thus, it is recommended that treatment of active injection drug use be considered on a case-by-case basis, and that active injection drug use in and of itself not be used to exclude such patients from antiviral therapy. HIV Co-infection Although there are no HCV therapies specifically approved for patients co-infected with HIV, these patients should be considered for treatment. Alcohol and HCV Alcohol is an important cofactor in the progression ofHCV liver disease to cirrhosis and HCC. A history of alcohol abuse is not a contraindication to therapy; however, continued alcohol use during therapy adversely affects response to treatment, and alcohol abstinence is strongly recommended before and during antiviral therapy. Heavy alcohol consumption of >80 g/day seriously compromises HCV treatment. Furthermore, safe levels of alcohol consumption are still unclear, and even moderate levels of consumption may accelerate disease progression in some patients. Recommendations to be made to patients to prevent transmission of hepatitis C The large reservoir of individuals infected with HCV provides a source of transmission to others at risk. Direct percutaneous exposure is the most efficient method for transmitting HCV, and injection drug use accounts for more than two-thirds of all new infections in the United States. Methadone treatment programs, needle and syringe exchange programs, and comprehensive risk-modifying educational programs have been shown to be effective in preventing HIV transmission and are likely to be useful for decreasing HCV transmission. Ensuring access to sterile syringes through physician prescription and pharmacy sales of syringes to roUs can also be helpful. roUs should be educated about the importance of hand washing before and after giving injections, not using the others' injection equipment, and avoiding any contact with blood from other persons. HCY prevention education should be a high priority in correctional settings. In the United States, the estimated seroprevalence of HCV is 2 to 3 percent among partners of HCV-infected persons who are in long-term monogamous relationships and is 4 to 6 percent among persons with multiple sex partners, sex workers, and men who have sex with men (those at risk for sexually transmitted diseases). One study found the risk of HCV infection to be threefold higher for female than male sexual partners. Because of the low risk of HCV transmission, monogamous couples do not need to use barrier protection (condoms) although they should be advised that condoms may reduce the risk of transmission. There is no evidence that kissing, hugging, sneezing, coughing, food, Hepatitis C Position Statement - Alabama Department of Corrections Summary ofNlli Statement Page 7 of8 February, 2003 water, sharing eating utensils or drinking glasses, casual contact, or other contact without exposure to blood is associated with HCV transmission for correctional staff. Body piercing and tattooing are other potential sources of transmission if contaminated equipment or supplies are used. However, transmission through these activities is rare and confounded by other risk factors. RECOMMENDATIONS ~ Educate the Ame11canpublic on the transmission of HCV in order to better identify affected individualsand to institutepreventivemeasures. ~ Promote the establishment of screening tests for all groups at high risk of HCV infection, including IDUs and incarcerated individuals. ~ Institute measures to reduce transmission of HCV among IDUs, including providing access to sterile syringes through needle exchange, physician prescription, and pharmacy sales; and expanding the Nation's capacity to provide treatment for substance abuse. Physicians and pharmacists should be educated to recognize that providing mus with access to sterile syringes and education in safe injection practices may be lifesaving. ~ Encourage a comprehensive approach to promote the collaboration among health professionals concerned with management of addiction. Primary care physicians, and specialists should be involved in various aspects of HCV management - to deal with the complex societal, medical, and psychiatri-c issues of mus afflicted by the disease.