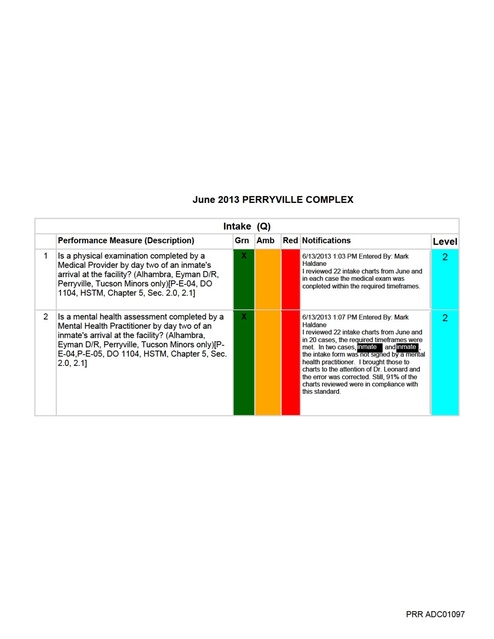
PRR ADC01097-01130 - Monthly Compliance Rpts - 2013-06 - ASPC-Perryville (redacted), AZ DOC, 2013
Download original document:
Document text
Document text
This text is machine-read, and may contain errors. Check the original document to verify accuracy.
June 2013 PERRYVILLE COMPLEX Responsible Parties = FHA/DON/RDCQI/RVP Target Date-11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 5 Are referrals to providers from sick call being seen within seven (7) days? [P-E-07] Level 1 Amber User: Mark Haldane Date: 6/28/2013 1:27:52 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.In-service all staff including providers on Sick Call 2.20.2.2 contract performance outcome 5 (Sick Call Attachment); Seen by Physician or Midlevel within 7 days a.Agenda/sign off sheet to verify 2.Monitoring (Sick Call Monitoring Tool) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties = FHA/DON/Medical Director/RDCQI/RVP Target Date- 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. PRR ADC01100 June 2013 PERRYVILLE COMPLEX 2 Are consultation reports being reviewed by the provider within seven (7) days of receipt? [CC 2.20.2.3] Level 2 Amber User: Vanessa Headstream Date: 6/27/2013 11:00:32 AM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.Standardized monitoring process 2.Communicate expectations via FHA/DON at quarterly training Regional office and obtain sign off sheet to verify 3.Monitoring (UM Audit Tool) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties =ARMD/RDON/RVP/RDCQI/DON/ Target Date-11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. PRR ADC01103 June 2013 PERRYVILLE COMPLEX a. Audit tools developed. b. Weekly site results discussed with RVP. c. Audit results discussed a monthly CQI meeting. d. Minutes and audit reported monthly to Regional office for tracking and trending. Responsible Parties = FHA/DON//Medical Director/RDCQI/RVP Target Date - 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 2 Are CC inmates being seen by the provider (every three (3) to six (6) months) as specified in the inmate’s treatment plan? [P-G-01, DO 1101, HSTM Chpt. 5, Sec. 5.1, CC 2.20.2.4] Level 2 Amber User: Vanessa Headstream Date: 6/27/2013 12:31:15 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by CorizonProcess statewide to include, but not limited to : 1. Chronic Care inmates seen by provider every 3-6 months, as specified in the treatment plan per Chronic Condition and Disease Management Programs 2.20.2.4 contract performance outcome 2 (I.- IV.Chronic Care Attachment). 2. In-service staff on policy titled ”Treatment Plans” Chapter 5, Section 1.4 (Appendix II.2.) and outcome measure . a. Agenda/sign off sheet to verify, inclusive of all pertinent staff . 3. Monitoring a. Audit tools developed. b. Weekly site results discussed with RVP. c. Audit results discussed a monthly CQI meeting. d. Minutes and audit reported monthly to Regional office for tracking and trending. Responsible Parties = FHA/DON//Medical Director/RDCQI/RVP Target Date - 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 3 Are CC/DM inmates being provided coaching and education about their condition / disease and is it documented in the medical record? [P-G-01, CC 2.20.2.4] Level 1 Amber User: Vanessa Headstream Date: 6/27/2013 12:31:55 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1. Standardized process for documenting in medical record chronic condition education per Chronic Condition and Disease Management Programs 2.20.2.4 contract performance outcome 3. 2. In-service staff on: a. Documentation of chronic condition education at each visit. b. Agenda/sign off sheet to verify, inclusive of all pertinent staff. 3. Monitoring a. Audit tools developed. b. Weekly site results discussed with RVP. c. Audit results discussed a monthly CQI meeting. d. Minutes and audit reported monthly to Regional office for tracking and trending. Responsible Parties = FHA/DON//Medical Director/RDCQI/RVP Target Date - 11/30/13 Plan weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results.10/11/13 Update – Documentation on education sheet located in front of chart, medical records responsible for making sure in chart. 3 Are CC/DM inmates being provided coaching and education about their condition / disease and is it documented in the medical record? [P-G-01, CC 2.20.2.4] Level 1 Amber User: Vanessa Headstream Date: 6/27/2013 12:31:55 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1. Standardized process for documenting in medical record chronic condition education per PRR ADC01106 June 2013 PERRYVILLE COMPLEX Chronic Condition and Disease Management Programs 2.20.2.4 contract performance outcome 3. 2. In-service staff on: a. Documentation of chronic condition education at each visit. b. Agenda/sign off sheet to verify, inclusive of all pertinent staff. 3. Monitoring a. Audit tools developed. b. Weekly site results discussed with RVP. c. Audit results discussed a monthly CQI meeting. d. Minutes and audit reported monthly to Regional office for tracking and trending. Responsible Parties = FHA/DON//Medical Director/RDCQI/RVP Target Date - 11/30/13 Plan weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results.10/11/13 Update – Documentation on education sheet located in front of chart, medical records responsible for making sure in chart. PRR ADC01107 June 2013 PERRYVILLE COMPLEX b.Re-order medications c.Invalid chart orders (Appendix I.1.c.) i.Therapeutic dose ranges ii.Dose changes must have supporting documentation d.Non-formulary process (Appendix I.1.d.) i.Reviewed for approval within 24-48 hrs ii.Providers notified decision within 24-48 hrs e.Manifest Reconciliation f.Inventory control g.Stock Medications h.Practitioner Cards (Appendis I.1.h.) i.Controlled Medications (Appendix I.1.i.) 2.In-service staff a.Using information from 8/19 - 11/13 Regional office mandatory in-service and PharmaCorr policy b.Agenda/sign off sheet to verify, inclusive of all pertinent staff (Appendix I.2.b.) 3.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties = FHA/DON/IC/RDCQI/RVP Target Date-11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 10/11/13 Update – Statewide in Sept Redbook and MAR audit, results reviewed; to audit pharmacy in October related to Controlled Substances and Expired meds. PRR ADC01109 June 2013 PERRYVILLE COMPLEX Target Date- 11/30/13 Continue to monitor daily, then monthly until meet compliance, then ongoing monthly monitoring. 10/11/13 Update: Staff in-serviced on how to use SMI monthly report tool; review of audit tool data to begin in November. 5 Are inmates prescribed psychotropic meds seen by a Psychiatrist or Psychiatric Mid-level Provider at a minimum of every three (3) months (90 days)?[CC 2.20.2.10] Level 2 Amber User: Steve Bender Date: 6/27/2013 12:47:45 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.Monitoring (Mental Health Monitoring Tool) a.Audit tools developed b.Monthly site results discussed with RVP/MH Director c.Audit results discussed at monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties = RDCQI/RVP/MH Director/FHA/DON/MH Lead Target Date- 11/30/13 Continue to monitor monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. PRR ADC01113 June 2013 PERRYVILLE COMPLEX Corrective Actions: Reinforce that the need for monthly reports identified in Exhibit 2 of the health services contract are being submitted in accordance with the contract. PRR ADC01115 June 2013 PERRYVILLE COMPLEX Corrective Action Plans for PerformanceMeasure: Medication Administration 2 Is the documentation of completed training and testing kept on file for staff who administer or deliver medications? [NCCHC Standard P-C-05; HSTM Chapter 3, Section 4.1] Level 1 Amber User: Vanessa Headstream Date: 6/28/2013 11:03:42 AM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.Standardized process statewide to include, but not limited to : a.Refusals/No Show - Policy titled “Appointment or Treatment Refusals” Chapter 5, Section 7.2 (Appendix VI.1.a.). b.MAR documentation. c.Administration of DOT/KOP. d.Printing MARs (Pharmacy Appendix). e.Medication error documentation/reporting (Pharmacy Appendix). 2.In-service staff on process and PharmaCorr policy. a.Agenda/sign off sheet to verify, inclusive of all pertinent staff. 3.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed. b.Weekly site results discussed with RVP. c.Audit results discussed a monthly CQI meeting. d.Minutes and audit reported monthly to Regional office for tracking and trending. Responsible Parties =FHA/DON/RDCQI/RVP/FHA Target Date- 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 4 Are the Medication Administration Records (MAR) being completed in accordance with standard nursing practices? [HSTM Chapter 4, Section 1.1, Chapter 5, Section 6.4] Level 1 Amber User: Vanessa Headstream Date: 6/18/2013 12:47:02 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.Standardized process statewide to include, but not limited to : a.Refusals/No Show - Policy titled “Appointment or Treatment Refusals” Chapter 5, Section 7.2 (Appendix VI.1.a.). b.MAR documentation. c.Administration of DOT/KOP. d.Printing MARs (Pharmacy Appendix). e.Medication error documentation/reporting (Pharmacy Appendix). 2.In-service staff on process and PharmaCorr policy. a.Agenda/sign off sheet to verify, inclusive of all pertinent staff. 3.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed. b.Weekly site results discussed with RVP. c.Audit results discussed a monthly CQI meeting. d.Minutes and audit reported monthly to Regional office for tracking and trending. Responsible Parties =FHA/DON/RDCQI/RVP/FHA Target Date- 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 4 Are the Medication Administration Records (MAR) being completed in accordance with standard nursing practices? [HSTM Chapter 4, Section 1.1, Chapter 5, Section 6.4] Level 1 Amber User: Vanessa Headstream Date: 6/18/2013 12:47:02 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.Standardized process statewide to include, but not limited to : a.Refusals/No Show - Policy titled “Appointment or Treatment Refusals” Chapter 5, Section 7.2 (Appendix VI.1.a.). b.MAR documentation. PRR ADC01120 June 2013 PERRYVILLE COMPLEX c.Administration of DOT/KOP. d.Printing MARs (Pharmacy Appendix). e.Medication error documentation/reporting (Pharmacy Appendix). 2.In-service staff on process and PharmaCorr policy. a.Agenda/sign off sheet to verify, inclusive of all pertinent staff. 3.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed. b.Weekly site results discussed with RVP. c.Audit results discussed a monthly CQI meeting. d.Minutes and audit reported monthly to Regional office for tracking and trending. Responsible Parties =FHA/DON/RDCQI/RVP/FHA Target Date- 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 4 Are the Medication Administration Records (MAR) being completed in accordance with standard nursing practices? [HSTM Chapter 4, Section 1.1, Chapter 5, Section 6.4] Level 1 Amber User: Vanessa Headstream Date: 6/18/2013 12:47:02 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.Standardized process statewide to include, but not limited to : a.Refusals/No Show - Policy titled “Appointment or Treatment Refusals” Chapter 5, Section 7.2 (Appendix VI.1.a.). b.MAR documentation. c.Administration of DOT/KOP. d.Printing MARs (Pharmacy Appendix). e.Medication error documentation/reporting (Pharmacy Appendix). 2.In-service staff on process and PharmaCorr policy. a.Agenda/sign off sheet to verify, inclusive of all pertinent staff. 3.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed. b.Weekly site results discussed with RVP. c.Audit results discussed a monthly CQI meeting. d.Minutes and audit reported monthly to Regional office for tracking and trending. Responsible Parties =FHA/DON/RDCQI/RVP/FHA Target Date- 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 4 Are the Medication Administration Records (MAR) being completed in accordance with standard nursing practices? [HSTM Chapter 4, Section 1.1, Chapter 5, Section 6.4] Level 1 Amber User: Vanessa Headstream Date: 6/18/2013 12:47:02 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.Standardized process statewide to include, but not limited to : a.Refusals/No Show - Policy titled “Appointment or Treatment Refusals” Chapter 5, Section 7.2 (Appendix VI.1.a.). b.MAR documentation. c.Administration of DOT/KOP. d.Printing MARs (Pharmacy Appendix). e.Medication error documentation/reporting (Pharmacy Appendix). 2.In-service staff on process and PharmaCorr policy. a.Agenda/sign off sheet to verify, inclusive of all pertinent staff. 3.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed. b.Weekly site results discussed with RVP. c.Audit results discussed a monthly CQI meeting. d.Minutes and audit reported monthly to Regional office for tracking and trending. Responsible Parties =FHA/DON/RDCQI/RVP/FHA PRR ADC01121 June 2013 PERRYVILLE COMPLEX Target Date- 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 5 Are medication errors forwarded to the FHA to review corrective action plan? Level 2 Amber User: Vanessa Headstream Date: 6/27/2013 11:10:59 AM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.Standardized process statewide to include, but not limited to : a.Medication error documentation/reporting (Pharmacy Appendix). 2.In-service staff on process and PharmaCorr policy. a.Agenda/sign off sheet to verify, inclusive of all pertinent staff. 3.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed. b.Weekly site results discussed with RVP. c.Audit results discussed a monthly CQI meeting. d.Minutes and audit reported monthly to Regional office for tracking and trending. Responsible Parties =FHA/DON/RDCQI/RVP/FHA Target Date- 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 6 Are there any unreasonable delays in inmate receiving prescribed medications? Level 2 Amber User: Vanessa Headstream Date: 6/18/2013 12:44:23 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by CorizonIntakes1.Standardized process for meds to be available to inmate upon transfer (Pharmacy Appendix 1 & 2) a.Intake Orders b.Private Prisons 2.In-service staff on process per PharmaCorr policy, a.Agenda/sign off sheet to verify, inclusive of all pertinent staff 3.Custody educated regarding contract requirements regarding inmate transfer with meds. 4.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsibile Parties = FHA/DON/Custody/RDCQI/RVP Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results 1.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending 2.Standardized process statewide to include, but not limited to (Appendix III.1.): a.Internal b.External 2.In-service staff on process and ADC policy titled “Continuity of Care Upon Transfer” Chapter 5, Section 5.0 (Appendices III.2.); a.Agenda/sign off sheet to verify, inclusive of all pertinent staff 3.Custody educated regarding contract requirements regarding inmate transfer with meds 4.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties = FHA/DON/Custody/RDCQI/RVP PRR ADC01122 June 2013 PERRYVILLE COMPLEX Target Date - 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 6 Are there any unreasonable delays in inmate receiving prescribed medications? Level 2 Amber User: Vanessa Headstream Date: 6/18/2013 12:44:23 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by CorizonIntakes1.Standardized process for meds to be available to inmate upon transfer (Pharmacy Appendix 1 & 2) a.Intake Orders b.Private Prisons 2.In-service staff on process per PharmaCorr policy, a.Agenda/sign off sheet to verify, inclusive of all pertinent staff 3.Custody educated regarding contract requirements regarding inmate transfer with meds. 4.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsibile Parties = FHA/DON/Custody/RDCQI/RVP Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results 1.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending 2.Standardized process statewide to include, but not limited to (Appendix III.1.): a.Internal b.External 2.In-service staff on process and ADC policy titled “Continuity of Care Upon Transfer” Chapter 5, Section 5.0 (Appendices III.2.); a.Agenda/sign off sheet to verify, inclusive of all pertinent staff 3.Custody educated regarding contract requirements regarding inmate transfer with meds 4.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties = FHA/DON/Custody/RDCQI/RVP Target Date - 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 6 Are there any unreasonable delays in inmate receiving prescribed medications? Level 2 Amber User: Vanessa Headstream Date: 6/18/2013 12:44:23 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by CorizonIntakes1.Standardized process for meds to be available to inmate upon transfer (Pharmacy Appendix 1 & 2) a.Intake Orders b.Private Prisons 2.In-service staff on process per PharmaCorr policy, a.Agenda/sign off sheet to verify, inclusive of all pertinent staff 3.Custody educated regarding contract requirements regarding inmate transfer with meds. 4.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP PRR ADC01123 June 2013 PERRYVILLE COMPLEX c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsibile Parties = FHA/DON/Custody/RDCQI/RVP Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results 1.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending 2.Standardized process statewide to include, but not limited to (Appendix III.1.): a.Internal b.External 2.In-service staff on process and ADC policy titled “Continuity of Care Upon Transfer” Chapter 5, Section 5.0 (Appendices III.2.); a.Agenda/sign off sheet to verify, inclusive of all pertinent staff 3.Custody educated regarding contract requirements regarding inmate transfer with meds 4.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties = FHA/DON/Custody/RDCQI/RVP Target Date - 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 8 Are chronic condition medication expiration dates being reviewed prior to expiration to ensure continuity of care? [NCCHC Standard P-D-01] Level 2 Amber User: Vanessa Headstream Date: 6/19/2013 3:35:17 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.Standardized process for meds to be available to inmate upon transfer (Pharmacy Appendix 1 & 2) 2.In-service staff on process per PharmaCorr policy, a.Agenda/sign off sheet to verify, inclusive of all pertinent staff 3.Custody educated regarding contract requirements regarding inmate transfer with meds. 4.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsibile Parties = FHA/DON/Custody/RDCQI/RVP Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results 1.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending 2.Standardized process statewide to include, but not limited to (Appendix III.1.): a.Internal b.External 2.In-service staff on process and ADC policy titled “Continuity of Care Upon Transfer” Chapter 5, Section 5.0 (Appendices III.2.); a.Agenda/sign off sheet to verify, inclusive of all pertinent staff 3.Custody educated regarding contract requirements regarding inmate transfer with meds 4.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed PRR ADC01124 June 2013 PERRYVILLE COMPLEX b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties = FHA/DON/Custody/RDCQI/RVP Target Date - 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 9 Are non-formulary requests being reviewed for approval or disapproval within 24 to 48 hours? Level 2 Amber User: Vanessa Headstream Date: 6/27/2013 11:11:56 AM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.Standardized process statewide, to include but not limited to (Pharmacy Appendix 1 & 2): a.Non-formulary process (Appendix I.1.d.) i.Reviewed for approval within 24-48 hrs ii.Providers notified decision within 24-48 hrs e.Manifest Reconciliation f.Inventory control g.Stock Medications h.Practitioner Cards (Appendis I.1.h.) i.Controlled Medications (Appendix I.1.i.) 2.In-service staff a.Using information from 8/19 - 11/13 Regional office mandatory in-service and PharmaCorr policy b.Agenda/sign off sheet to verify, inclusive of all pertinent staff (Appendix I.2.b.) 3.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties = FHA/DON/IC/RDCQI/RVP Target Date-11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 10/11/13 Update – Statewide in Sept Redbook and MAR audit, results reviewed; to audit pharmacy in October related to Controlled Substances and Expired meds. 9 Are non-formulary requests being reviewed for approval or disapproval within 24 to 48 hours? Level 2 Amber User: Vanessa Headstream Date: 6/27/2013 11:11:56 AM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.Standardized process statewide, to include but not limited to (Pharmacy Appendix 1 & 2): a.Non-formulary process (Appendix I.1.d.) i.Reviewed for approval within 24-48 hrs ii.Providers notified decision within 24-48 hrs e.Manifest Reconciliation f.Inventory control g.Stock Medications h.Practitioner Cards (Appendis I.1.h.) i.Controlled Medications (Appendix I.1.i.) 2.In-service staff a.Using information from 8/19 - 11/13 Regional office mandatory in-service and PharmaCorr policy b.Agenda/sign off sheet to verify, inclusive of all pertinent staff (Appendix I.2.b.) 3.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending PRR ADC01125 June 2013 PERRYVILLE COMPLEX Responsible Parties = FHA/DON/IC/RDCQI/RVP Target Date-11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 10/11/13 Update – Statewide in Sept Redbook and MAR audit, results reviewed; to audit pharmacy in October related to Controlled Substances and Expired meds. 10 Are providers being notified of non-formulary decisions within 24 to 48 hours? Level 2 Amber User: Vanessa Headstream Date: 6/24/2013 1:19:36 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.Standardized process statewide, to include but not limited to (Pharmacy Appendix 1 & 2): a.Non-formulary process (Appendix I.1.d.) i.Reviewed for approval within 24-48 hrs ii.Providers notified decision within 24-48 hrs e.Manifest Reconciliation f.Inventory control g.Stock Medications h.Practitioner Cards (Appendis I.1.h.) i.Controlled Medications (Appendix I.1.i.) 2.In-service staff a.Using information from 8/19 - 11/13 Regional office mandatory in-service and PharmaCorr policy b.Agenda/sign off sheet to verify, inclusive of all pertinent staff (Appendix I.2.b.) 3.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties = FHA/DON/IC/RDCQI/RVP Target Date-11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 10/11/13 Update – Statewide in Sept Redbook and MAR audit, results reviewed; to audit pharmacy in October related to Controlled Substances and Expired meds. 11 Are medication error reports being completed and medication errors documented? Level 2 Amber User: Vanessa Headstream Date: 6/27/2013 11:13:18 AM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.Standardized process statewide to include, but not limited to : a.Medication error documentation/reporting (Pharmacy Appendix). 2.In-service staff on process and PharmaCorr policy. a.Agenda/sign off sheet to verify, inclusive of all pertinent staff. 3.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed. b.Weekly site results discussed with RVP. c.Audit results discussed a monthly CQI meeting. d.Minutes and audit reported monthly to Regional office for tracking and trending. Responsible Parties =FHA/DON/RDCQI/RVP/FHA Target Date- 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. PRR ADC01126