PRR ADC01428-01466 - Monthly Compliance Rpts - 2013-07 - ASPC-Phoenix (redacted), AZ DOC, 2013
Download original document:
Document text
Document text
This text is machine-read, and may contain errors. Check the original document to verify accuracy.
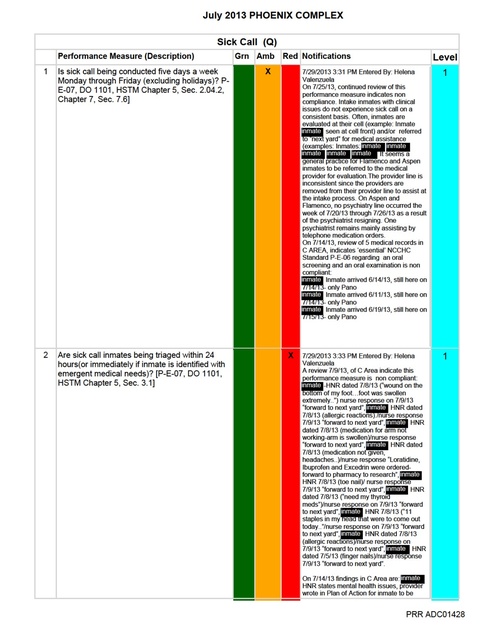
July 2013 PHOENIX COMPLEX Corrective Action Plans for PerformanceMeasure: Sick Call (Q) 1 Is sick call being conducted five days a week Monday through Friday (excluding holidays)? P-E-07, DO 1101, HSTM Chapter 5, Sec. 2.04.2, Chapter 7, Sec. 7.6] Level 1 Amber User: Helena Valenzuela Date: 7/29/2013 3:30:42 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.Process to address access to care, to include but not limited to: a.Scheduling patients b.Staffing 2.In-service staff on process expectations per Sick Call 2.20.2.2 contract performance outcome 1 Sick call shall be held five days a week, Monday through Friday (excluding Holidays), for all inmates (Sick Call Attachment); and site specific process a.Agenda/sign off sheet to verify, inclusive of all pertinent staff 3.Monitoring (Sick Call Audit Tool) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties = FHA/DON/RDCQI/RVP Target Date-11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 10/11/13 Update – All HNR s to be triaged by nursing, inclusive of MH. 2 Are sick call inmates being triaged within 24 hours(or immediately if inmate is identified with emergent medical needs)? [P-E-07, DO 1101, HSTM Chapter 5, Sec. 3.1] Level 1 Red User: Helena Valenzuela Date: 7/29/2013 3:32:36 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.Process to address, to include but not limited to: a.Daily pick up. b.Date stamp. c.Triage within 24 hrs, immediate triage of patient if emergent. d.Seen within 48 hrs after date stamp or 72 hrs weekend/holiday. e.Nurse line sees patient, then to provider line when appropriate. f. Submit final site process to RVP. 2.In-service staff on policy titled ”Routine Appointments – Request” Chapter 5, Section 3.1 ( (Attachment II.2.) and per Sick Call 2.20.2.2 contract performance outcome 2 (Sick Call Attachment); a.Agenda/sign off sheet to verify, inclusive of all pertinent staff. 3.Monitoring (Sick Call Monitoring Tool) a.Audit tools developed. b.Weekly site results discussed with RVP. c.Audit results discussed a monthly CQI meeting. d.Minutes and audit reported monthly to Regional office for tracking and trending. Responsible Parties = FHA/DON/RDCQI/RVP Target Date-11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 3 Are vitals signs, to include weight, being checked and documented each time an inmate is seen during sick call? [P-E-04, HSTM Chapter 5, Section 1.3] Level 1 Amber User: Helena Valenzuela Date: 7/29/2013 3:33:19 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.In-service nursing staff on per Sick Call 2.20.2.2 contract performance outcome 3 (Sick Call Attachment); a.Agenda/sign off sheet to verify PRR ADC01433 July 2013 PHOENIX COMPLEX 2.Monitoring (Sick Call Monitoring Tool) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties = FHA/DON/RDCQI/RVP Target Date- 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 10/11/13 Update – VS will include weight when appropriate. 4 Is the SOAPE format being utilized in the inmate medical record for encounters? [DO 1104, HSTM Chapter 5, Section 1.3] Level 1 Amber User: Helena Valenzuela Date: 7/29/2013 3:34:06 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.In-service all staff including providers on policy titled ”Continuous Progress Note (SOAP)”, Chapter 5, Section 1.3 (Attachment IV.1.) and per Sick Call 2.20.2.2 contract performance outcome 4 (Sick Call Attachment); use of Corizon NETs a.Agenda/sign off sheet to verify 2.Monitoring (Sick Call Monitoring Tool) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties = FHA/DON/Medical Director/RDCQI/RVP Target Date- 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 10/11/13 Update –NETs to be used for all Nursing sick call. 5 Are referrals to providers from sick call being seen within seven (7) days? [P-E-07] Level 1 Red User: Helena Valenzuela Date: 7/31/2013 4:03:05 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.In-service all staff including providers on Sick Call 2.20.2.2 contract performance outcome 5 (Sick Call Attachment); Seen by Physician or Midlevel within 7 days a.Agenda/sign off sheet to verify 2.Monitoring (Sick Call Monitoring Tool) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties = FHA/DON/Medical Director/RDCQI/RVP Target Date- 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 6 Are nursing protocols in place and utilized by the nurses for sick call? Level 1 Amber User: Helena Valenzuela Date: 7/29/2013 3:37:48 PM Corrective Plan: 9/9/13 - Nursing Encounter Tools are used with standing orders that can be located in the NETs binder found on every unit. These forms are to be used with every nursing-inmate encounter. The process of completeing Nursing Encounter Tools, (NETs), will continue to be reviewed on a monthly and ad lib basis. Corrective Actions: See above. PRR ADC01434 July 2013 PHOENIX COMPLEX a. Approved consults scheduled/documented within 5 days by clinical coordinator 2. Schedule and conduct training for all clinical coordinators a.Agenda/sign off sheet to verify 3. Monitoring (UM Audit Tool) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsibile Parties = DON/Clinical Systems Business Analyst II/FHA/DON/RDCQI/RVP Target Date - 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 2 Are consultation reports being reviewed by the provider within seven (7) days of receipt? [CC 2.20.2.3] Level 2 Amber User: Vanessa Headstream Date: 7/26/2013 11:27:20 AM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.Standardized monitoring process 2.Communicate expectations via FHA/DON at quarterly training Regional office and obtain sign off sheet to verify 3.Monitoring (UM Audit Tool) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties =ARMD/RDON/RVP/RDCQI/DON/ Target Date-11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. PRR ADC01436 July 2013 PHOENIX COMPLEX d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties = FHA/DON/IC/RDCQI/RVP Target Date-11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 10/11/13 Update – Statewide in Sept Redbook and MAR audit, results reviewed; to audit pharmacy in October related to Controlled Substances and Expired meds. PRR ADC01439 July 2013 PHOENIX COMPLEX Corrective Action Plans for PerformanceMeasure: Intake (Reception) 8 Are inmate prescribed medications transferred with a 45 day supply? Alhambra, Perryville, Tucson Minors only [HSTM Chapter 5, Section 6.1 and CC 2.12.22] Level 1 Amber User: Helena Valenzuela Date: 7/29/2013 3:19:38 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: Reinforce to staff ADC Policy that inmate prescribed medications must be transferred with a 45 day supply. PRR ADC01443 July 2013 PHOENIX COMPLEX Corrective Action Plans for PerformanceMeasure: Medication Administration 2 Is the documentation of completed training and testing kept on file for staff who administer or deliver medications? [NCCHC Standard P-C-05; HSTM Chapter 3, Section 4.1] Level 1 Amber User: Vanessa Headstream Date: 7/31/2013 2:00:39 PM Corrective Plan: All requested information sent same day as requested. 8/16/13 - Answer is final. Corizon policies followed and informstion sent same day as requested. See below. Corrective Actions: October Action plan submitted by Corizon1.Standardized process statewide to include, but not limited to : a.Refusals/No Show - Policy titled “Appointment or Treatment Refusals” Chapter 5, Section 7.2 (Appendix VI.1.a.). b.MAR documentation. c.Administration of DOT/KOP. d.Printing MARs (Pharmacy Appendix). e.Medication error documentation/reporting (Pharmacy Appendix). 2.In-service staff on process and PharmaCorr policy. a.Agenda/sign off sheet to verify, inclusive of all pertinent staff. 3.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed. b.Weekly site results discussed with RVP. c.Audit results discussed a monthly CQI meeting. d.Minutes and audit reported monthly to Regional office for tracking and trending. Responsible Parties =FHA/DON/RDCQI/RVP/FHA Target Date- 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 4 Are the Medication Administration Records (MAR) being completed in accordance with standard nursing practices? [HSTM Chapter 4, Section 1.1, Chapter 5, Section 6.4] Level 1 Amber User: Vanessa Headstream Date: 7/31/2013 2:37:16 PM Corrective Plan: Problem Identified: Incomplete MARs Discussion and Action Plan: As a result of this finding, the FHA and DON have instituted a process of confirming that all medications currently prescribed for patients have an accurate MAR. The 26th of each month prior to the printing of the MARs, the DON shall run a census (through AIMS) of all inmates in designated housing areas (excluding intakes) and distribute this census to the nursing staff responsible for those areas. Nursing staff shall then do a chart review of each patient and confirm that MARs are accurate and present in the MAR books. Nurses shall notate on the census report if MARs are present and accurate and shall immediately correct or replace any missing or inaccurate MARs. At the completion of this task, the census report shall be delivered back to the DON for review and a copy of this report shall be maintained in the DON's office for compliance inspection by contract monitors. These reports shall be made available on the second Monday of each month. Inventory coordinators may assist in this task as supervised by nursing staff. Responsible Person: Nursing staff assigned to units for task completion. DON for review and training. FHA for process implementation/development/direction. Status: Initial reviews will begin immediately and the formal process is to begin August 2013. First reports with any luck will be available on August 12th. See below. CAP Revision #1 - It is illegal to back chart, so the records cannot be altered. All we can do is focus on prevention, education and monitoring. Training and increased observation by leadership is the focus. 8/15/13 - The answer provided is final. Corrective Actions: October Action plan submitted by Corizon1.Standardized process statewide to include, but not limited to : PRR ADC01450 July 2013 PHOENIX COMPLEX a.Refusals/No Show - Policy titled “Appointment or Treatment Refusals” Chapter 5, Section 7.2 (Appendix VI.1.a.). b.MAR documentation. c.Administration of DOT/KOP. d.Printing MARs (Pharmacy Appendix). e.Medication error documentation/reporting (Pharmacy Appendix). 2.In-service staff on process and PharmaCorr policy. a.Agenda/sign off sheet to verify, inclusive of all pertinent staff. 3.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed. b.Weekly site results discussed with RVP. c.Audit results discussed a monthly CQI meeting. d.Minutes and audit reported monthly to Regional office for tracking and trending. Responsible Parties =FHA/DON/RDCQI/RVP/FHA Target Date- 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 4 Are the Medication Administration Records (MAR) being completed in accordance with standard nursing practices? [HSTM Chapter 4, Section 1.1, Chapter 5, Section 6.4] Level 1 Amber User: Vanessa Headstream Date: 7/31/2013 2:37:16 PM Corrective Plan: Problem Identified: Incomplete MARs Discussion and Action Plan: As a result of this finding, the FHA and DON have instituted a process of confirming that all medications currently prescribed for patients have an accurate MAR. The 26th of each month prior to the printing of the MARs, the DON shall run a census (through AIMS) of all inmates in designated housing areas (excluding intakes) and distribute this census to the nursing staff responsible for those areas. Nursing staff shall then do a chart review of each patient and confirm that MARs are accurate and present in the MAR books. Nurses shall notate on the census report if MARs are present and accurate and shall immediately correct or replace any missing or inaccurate MARs. At the completion of this task, the census report shall be delivered back to the DON for review and a copy of this report shall be maintained in the DON's office for compliance inspection by contract monitors. These reports shall be made available on the second Monday of each month. Inventory coordinators may assist in this task as supervised by nursing staff. Responsible Person: Nursing staff assigned to units for task completion. DON for review and training. FHA for process implementation/development/direction. Status: Initial reviews will begin immediately and the formal process is to begin August 2013. First reports with any luck will be available on August 12th. Corrective Actions: Approved. 4 Are the Medication Administration Records (MAR) being completed in accordance with standard nursing practices? [HSTM Chapter 4, Section 1.1, Chapter 5, Section 6.4] Level 1 Amber User: Vanessa Headstream Date: 7/31/2013 2:37:16 PM Corrective Plan: Problem Identified: Incomplete MARs Discussion and Action Plan: As a result of this finding, the FHA and DON have instituted a process of confirming that all medications currently prescribed for patients have an accurate MAR. The 26th of each month prior to the printing of the MARs, the DON shall run a census (through AIMS) of all inmates in designated housing areas (excluding intakes) and distribute this census to the nursing staff responsible for those areas. Nursing staff shall then do a chart review of each patient and confirm that MARs are accurate and present in the MAR books. Nurses shall notate on the census report if MARs are present and accurate and shall immediately correct or replace any missing or inaccurate MARs. At the completion of this task, the census report shall be delivered back to the DON for review and a copy of this report shall be maintained in the DON's office for compliance inspection by contract monitors. These reports shall be made available on the second Monday of each month. Inventory coordinators may assist in this task as supervised by nursing staff. Responsible Person: Nursing staff assigned to units for task completion. DON for review and training. FHA for process implementation/development/direction. PRR ADC01451 July 2013 PHOENIX COMPLEX Status: Initial reviews will begin immediately and the formal process is to begin August 2013. First reports with any luck will be available on August 12th. Corrective Actions: Approved. 5 Are medication errors forwarded to the FHA to review corrective action plan? Level 2 Amber User: Vanessa Headstream Date: 7/31/2013 2:23:03 PM Corrective Plan: Problem Identified: Medication Error corrective action plan completion Discussion and Action Plan: As a result of this finding, the FHA has instititued a plan to ensure compliance. By COB on the last day of the month, the DON shall submit a medication error report to the FHA. This report shall be reviewed by the FHA and shall be available for review by monitors on the first Monday of the following month. Responsible Person: Nursing staff is responsible for submitting error reports to DON. DON is responsible for submitting compiled reports to FHA and for action on any medication errors. FHA is responsible for maintaining records and reporting of medication errors. Status: A formal process has been in place but this process shall begin 8/1/13. Anticipated Completion Date: Ongoing process that will require ongoing monitoring and as such, no date of completion can be given. Date Completed: See immediate previous response. Corrective Actions: CAP Revision #1 - Process worked out with Ms. Campbell today, that all future med errors will be scanned to Ms. Headstream as processed. 6 Are there any unreasonable delays in inmate receiving prescribed medications? Level 2 Amber User: Vanessa Headstream Date: 7/31/2013 2:20:32 PM Corrective Plan: See October action plan as submitted by Corizon. In process of gathering knowledge neede to respond, (MGAR won't let me close without a response, so I had to write in something?). Corrective Actions: October Action plan submitted by CorizonIntakes1.Standardized process for meds to be available to inmate upon transfer (Pharmacy Appendix 1 & 2) a.Intake Orders b.Private Prisons 2.In-service staff on process per PharmaCorr policy, a.Agenda/sign off sheet to verify, inclusive of all pertinent staff 3.Custody educated regarding contract requirements regarding inmate transfer with meds. 4.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsibile Parties = FHA/DON/Custody/RDCQI/RVP Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results 1.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending 2.Standardized process statewide to include, but not limited to (Appendix III.1.): a.Internal b.External 2.In-service staff on process and ADC policy titled “Continuity of Care Upon Transfer” Chapter 5, Section 5.0 (Appendices III.2.); a.Agenda/sign off sheet to verify, inclusive of all pertinent staff 3.Custody educated regarding contract requirements regarding inmate transfer with meds 4.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed PRR ADC01452 July 2013 PHOENIX COMPLEX b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties = FHA/DON/Custody/RDCQI/RVP Target Date - 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 6 Are there any unreasonable delays in inmate receiving prescribed medications? Level 2 Amber User: Vanessa Headstream Date: 7/31/2013 2:20:32 PM Corrective Plan: See October action plan as submitted by Corizon. In process of gathering knowledge neede to respond, (MGAR won't let me close without a response, so I had to write in something?). Corrective Actions: October Action plan submitted by CorizonIntakes1.Standardized process for meds to be available to inmate upon transfer (Pharmacy Appendix 1 & 2) a.Intake Orders b.Private Prisons 2.In-service staff on process per PharmaCorr policy, a.Agenda/sign off sheet to verify, inclusive of all pertinent staff 3.Custody educated regarding contract requirements regarding inmate transfer with meds. 4.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsibile Parties = FHA/DON/Custody/RDCQI/RVP Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results 1.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending 2.Standardized process statewide to include, but not limited to (Appendix III.1.): a.Internal b.External 2.In-service staff on process and ADC policy titled “Continuity of Care Upon Transfer” Chapter 5, Section 5.0 (Appendices III.2.); a.Agenda/sign off sheet to verify, inclusive of all pertinent staff 3.Custody educated regarding contract requirements regarding inmate transfer with meds 4.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties = FHA/DON/Custody/RDCQI/RVP Target Date - 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 8 Are chronic condition medication expiration dates being reviewed prior to expiration to ensure continuity of care? [NCCHC Standard P-D-01] Level 2 Amber User: Vanessa Headstream Date: 7/25/2013 2:48:15 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.Standardized process for meds to be available to inmate upon transfer (Pharmacy Appendix 1 & 2) 2.In-service staff on process per PharmaCorr policy, a.Agenda/sign off sheet to verify, inclusive of all pertinent staff 3.Custody educated regarding contract requirements regarding inmate transfer with meds. PRR ADC01453 July 2013 PHOENIX COMPLEX 4.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsibile Parties = FHA/DON/Custody/RDCQI/RVP Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results 1.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending 2.Standardized process statewide to include, but not limited to (Appendix III.1.): a.Internal b.External 2.In-service staff on process and ADC policy titled “Continuity of Care Upon Transfer” Chapter 5, Section 5.0 (Appendices III.2.); a.Agenda/sign off sheet to verify, inclusive of all pertinent staff 3.Custody educated regarding contract requirements regarding inmate transfer with meds 4.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties = FHA/DON/Custody/RDCQI/RVP Target Date - 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 9 Are non-formulary requests being reviewed for approval or disapproval within 24 to 48 hours? Level 2 Amber User: Vanessa Headstream Date: 7/26/2013 11:34:46 AM Corrective Plan: This process is in committee, as is a statewide Corizon/Pharmacorr issue. First committee meeting is Friday, August 2, 2013. 8/16/13 - Please refer this to Regional level. Site does not control Pharmacorr P&P. See below. Corrective Actions: October Action plan submitted by Corizon1.Standardized process statewide, to include but not limited to (Pharmacy Appendix 1 & 2): a.Non-formulary process (Appendix I.1.d.) i.Reviewed for approval within 24-48 hrs ii.Providers notified decision within 24-48 hrs e.Manifest Reconciliation f.Inventory control g.Stock Medications h.Practitioner Cards (Appendis I.1.h.) i.Controlled Medications (Appendix I.1.i.) 2.In-service staff a.Using information from 8/19 - 11/13 Regional office mandatory in-service and PharmaCorr policy b.Agenda/sign off sheet to verify, inclusive of all pertinent staff (Appendix I.2.b.) 3.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties = FHA/DON/IC/RDCQI/RVP Target Date-11/30/13 PRR ADC01454 July 2013 PHOENIX COMPLEX Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 10/11/13 Update – Statewide in Sept Redbook and MAR audit, results reviewed; to audit pharmacy in October related to Controlled Substances and Expired meds. 10 Are providers being notified of non-formulary decisions within 24 to 48 hours? Level 2 Amber User: Vanessa Headstream Date: 7/26/2013 11:35:11 AM Corrective Plan: This process is in committee, as is a statewide Corizon/Pharmacorr issue. First committee meeting is Friday, August 2, 2013. 8/16/13 - Please refer this to the Regional level. Site does not control Pharmacorr P7P. See below. Corrective Actions: October Action plan submitted by Corizon1.Standardized process statewide, to include but not limited to (Pharmacy Appendix 1 & 2): a.Non-formulary process (Appendix I.1.d.) i.Reviewed for approval within 24-48 hrs ii.Providers notified decision within 24-48 hrs e.Manifest Reconciliation f.Inventory control g.Stock Medications h.Practitioner Cards (Appendis I.1.h.) i.Controlled Medications (Appendix I.1.i.) 2.In-service staff a.Using information from 8/19 - 11/13 Regional office mandatory in-service and PharmaCorr policy b.Agenda/sign off sheet to verify, inclusive of all pertinent staff (Appendix I.2.b.) 3.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties = FHA/DON/IC/RDCQI/RVP Target Date-11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 10/11/13 Update – Statewide in Sept Redbook and MAR audit, results reviewed; to audit pharmacy in October related to Controlled Substances and Expired meds. 11 Are medication error reports being completed and medication errors documented? Level 2 Amber User: Vanessa Headstream Date: 7/31/2013 2:23:13 PM Corrective Plan: Problem Identified: Medication Error reporting on time Discussion and Action Plan: As a result of this finding, the FHA has instititued a plan to ensure compliance. By COB on the last day of the month, the DON shall submit a medication error report to the FHA. This report shall be reviewed by the FHA and shall be available for review by monitors on the first Monday of the following month. Responsible Person: Nursing staff is responsible for submitting error reports to DON. DON is responsible for submitting compiled reports to FHA and for action on any medication errors. FHA is responsible for maintaining records and reporting of medication errors. Status: A formal process has been in place but this process shall begin 8/1/13. Anticipated Completion Date: Ongoing process that will require ongoing monitoring and as such, no date of completion can be given. Date Completed: See immediate previous response. CAP Revision #1 - Process worked out with Ms. Campbell today, that all future med errors will be scanned to Ms. Headstream as processed. PRR ADC01455 July 2013 PHOENIX COMPLEX Corrective Actions: October Action plan submitted by Corizon1.Standardized process statewide to include, but not limited to : a.Medication error documentation/reporting (Pharmacy Appendix). 2.In-service staff on process and PharmaCorr policy. a.Agenda/sign off sheet to verify, inclusive of all pertinent staff. 3.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed. b.Weekly site results discussed with RVP. c.Audit results discussed a monthly CQI meeting. d.Minutes and audit reported monthly to Regional office for tracking and trending. Responsible Parties =FHA/DON/RDCQI/RVP/FHA Target Date- 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. PRR ADC01456 July 2013 PHOENIX COMPLEX Locums are used to cover vacancies. Corrective Actions: Approved. See above. PRR ADC01458 July 2013 PHOENIX COMPLEX Corrective Action Plans for PerformanceMeasure: Medication Room 1 Is the medical room kept locked when not occupied? Level 1 Amber User: Vanessa Headstream Date: 7/31/2013 2:34:43 PM Corrective Plan: Problem Identified: Medical room's not kept secured. Discussion and Action Plan: As a result of this finding, the FHA, Assistant FHA, and DON have sent a directive to all staff instructing them to ensure that doors to medical rooms be kept closed and locked in order to ensure compliance. The Assistant FHA or designee will make rounds on a daily basis to ensure that all med rooms are locked when not in use. A log of these rounds will be kept and maintained in the Assistant FHA's office and shall be available for review. Automatic door closers have been requested of ADC's physical plant/maintenance staff. Responsible Person: Assitant FHA (or designee) for daily rounds and log maintenance. FHA for process implementation/development/direction. Status: This process shall begin 8/1/13. Anticipated Completion Date: Ongoing process that will require ongoing monitoring and as such, no date of completion can be given. Date Completed: See immediate previous response. CAP Revision #1 - The narcotics have been taken to be stored on King/Quiet until our new lock comes in, (the company sent the keys but not the lock). Corrective Actions: See aove. 1 Is the medical room kept locked when not occupied? Level 1 Amber User: Vanessa Headstream Date: 7/31/2013 2:34:43 PM Corrective Plan: Problem Identified: Medical room's not kept secured. Discussion and Action Plan: As a result of this finding, the FHA, Assistant FHA, and DON have sent a directive to all staff instructing them to ensure that doors to medical rooms be kept closed and locked in order to ensure compliance. The Assistant FHA or designee will make rounds on a daily basis to ensure that all med rooms are locked when not in use. A log of these rounds will be kept and maintained in the Assistant FHA's office and shall be available for review. Responsible Person: Assitant FHA (or designee) for daily rounds and log maintenance. FHA for process implementation/development/direction. Status: This process shall begin 8/1/13. Anticipated Completion Date: Ongoing process that will require ongoing monitoring and as such, no date of completion can be given. Date Completed: See immediate previous response. CAP Revision #1 - The narcotics have been taken to be stored on King/Quiet until our new lock comes in, (the company sent the keys but not the lock). Corrective Actions: See above. 1 Is the medical room kept locked when not occupied? Level 1 Amber User: Vanessa Headstream Date: 7/31/2013 2:34:43 PM Corrective Plan: Problem Identified: Medical room's not kept secured. Discussion and Action Plan: As a result of this finding, the FHA, Assistant FHA, and DON have sent a directive to all staff instructing them to ensure that doors to medical rooms be kept closed and locked in order to ensure compliance. The Assistant FHA or designee will make rounds on a daily basis to ensure that all med rooms are locked when not in use. A log of these rounds will be kept and maintained in the Assistant FHA's office and shall be available for review. PRR ADC01463 July 2013 PHOENIX COMPLEX Responsible Person: Assitant FHA (or designee) for daily rounds and log maintenance. FHA for process implementation/development/direction. Status: This process shall begin 8/1/13. Anticipated Completion Date: Ongoing process that will require ongoing monitoring and as such, no date of completion can be given. Date Completed: See immediate previous response. CAP Revision #1 - The narcotics have been taken to be stored on King/Quiet until our new lock comes in, (the company sent the keys but not the lock). Corrective Actions: See above. 2 Are quarterly audits of the unit (Floor Stock/RDSA)medicaton by a pharmacist being conducted and documented? Level 2 Amber User: Vanessa Headstream Date: 7/25/2013 2:59:51 PM Corrective Plan: This process is in committee, as is a statewide Corizon/Pharmacorr issue. First committee meeting is Friday, August 2, 2013. This is not site specific. 8/16/13 - Regional Management confirmed the quarterly audit was done. Please see Regional Team for access to reports. Corrective Actions: See above. 2 Are open medication vials being marked with the date they were opened? Level 1 Amber User: Vanessa Headstream Date: 7/31/2013 2:26:19 PM Corrective Plan: Problem Identified: Marking medication vials. Discussion and Action Plan: As a result of this finding, the DON has instituted a process to ensure compliance. The DON has instructed the Medication Inventory Coordinators to, on a monthly basis, do an audit of all stock and vial medications. This audit is to include the medication name and the corresponding expiration date. Upon completion, the audit report is to be submitted to the DON for review and action. Copies of this report are maintained in the DON's office. Responsible Person: Medication Inventory Coordinators responsible for medication audits and report. DON is responsible for oversight and review of reports as well as actions required for proper medication disposal. Status: This process has been in place since June 2013. Anticipated Completion Date: As this is an ongoing process, no completion date can be given. Date Completed: See immediately previous response. CAP Revision #1 - We will trial doing those audits weekly, to monitor the effectiveness, for one month. Additionally, there was some confusion as to stop dates vs expiration dates, which Ms Headstream and Ms. Somner were happy to address. Corrective Actions: 9/12/13 addition to CAP: The Assistant Facility Health Administrator has been added to the inspection team. He will conduct two inspections per month approximately two weeks apart. He will check for stop dates, contraband within refrigerators, and out of date product. The AFHA completed his first walk through today (9/12/13. 2 Are open medication vials being marked with the date they were opened? Level 1 Amber User: Vanessa Headstream Date: 7/31/2013 2:26:19 PM Corrective Plan: Problem Identified: Marking medication vials. Discussion and Action Plan: As a result of this finding, the DON has instituted a process to ensure compliance. The DON has instructed the Medication Inventory Coordinators to, on a monthly basis, do an audit of all stock and vial medications. This audit is to include the medication name and the corresponding expiration date. Upon completion, PRR ADC01464 July 2013 PHOENIX COMPLEX the audit report is to be submitted to the DON for review and action. Copies of this report are maintained in the DON's office. Responsible Person: Medication Inventory Coordinators responsible for medication audits and report. DON is responsible for oversight and review of reports as well as actions required for proper medication disposal. Status: This process has been in place since June 2013. Anticipated Completion Date: As this is an ongoing process, no completion date can be given. Date Completed: See immediately previous response. CAP Revision #1 - We will trial doing those audits weekly, to monitor the effectiveness, for one month. Additionally, there was some confusion as to stop dates vs expiration dates, which Ms Headstream and Ms. Somner were happy to address. We were unable to identify the employee reported to have left food in the fridge. There are notes going up on the units today. Corrective Actions: See above. 2 Are open medication vials being marked with the date they were opened? Level 1 Amber User: Vanessa Headstream Date: 7/31/2013 2:26:19 PM Corrective Plan: Problem Identified: Marking medication vials. Discussion and Action Plan: As a result of this finding, the DON has instituted a process to ensure compliance. The DON has instructed the Medication Inventory Coordinators to, on a monthly basis, do an audit of all stock and vial medications. This audit is to include the medication name and the corresponding expiration date. Upon completion, the audit report is to be submitted to the DON for review and action. Copies of this report are maintained in the DON's office. Responsible Person: Medication Inventory Coordinators responsible for medication audits and report. DON is responsible for oversight and review of reports as well as actions required for proper medication disposal. Status: This process has been in place since June 2013. Anticipated Completion Date: As this is an ongoing process, no completion date can be given. Date Completed: See immediately previous response.CAP Revision #1 - We will trial doing those audits weekly, to monitor the effectiveness, for one month. Additionally, there was some confusion as to stop dates vs expiration dates, which Ms Headstream and Ms. Somner were happy to address. Corrective Actions: See above. 3 Is nursing staff checking for outdated (expiring)medications? Level 1 Amber User: Vanessa Headstream Date: 7/31/2013 2:33:57 PM Corrective Plan: Problem Identified: Checking outdates (expiring) medications. Discussion and Action Plan: As a result of this finding, the DON has instituted a process to ensure compliance. The DON has instructed the Medication Inventory Coordinators to, on a monthly basis, do an audit of all stock and vial medications. This audit is to include the medication name and the corresponding expiration date. Upon completion, the audit report is to be submitted to the DON for review and action. Copies of this report are maintained in the DON's office. Responsible Person: Medication Inventory Coordinators responsible for medication audits and report. DON is responsible for oversight and review of reports as well as actions required for proper medication disposal. Status: This process has been in place since June 2013. Anticipated Completion Date: As this is an ongoing process, no completion date can be given. Date Completed: See immediately previous response PRR ADC01465 July 2013 PHOENIX COMPLEX CAP Revision #1 - We will trial doing those audits weekly, to monitor the effectiveness, for one month. Additionally, there was some confusion as to stop dates vs expiration dates, which Ms Headstream and Ms. Somner were happy to address. Corrective Actions: 9/12/13 addition to CAP: The Assistant Facility Health Administrator has been added to the inspection team. He will conduct two inspections per month approximately two weeks apart. He will check for stop dates, contraband within refrigerators, and out of date product. The AFHA completed his first walk through today (9/12/13). 3 Is nursing staff checking for outdated (expiring)medications? Level 1 Amber User: Vanessa Headstream Date: 7/31/2013 2:33:57 PM Corrective Plan: Problem Identified: Checking outdates (expiring) medications. Discussion and Action Plan: As a result of this finding, the DON has instituted a process to ensure compliance. The DON has instructed the Medication Inventory Coordinators to, on a monthly basis, do an audit of all stock and vial medications. This audit is to include the medication name and the corresponding expiration date. Upon completion, the audit report is to be submitted to the DON for review and action. Copies of this report are maintained in the DON's office. Responsible Person: Medication Inventory Coordinators responsible for medication audits and report. DON is responsible for oversight and review of reports as well as actions required for proper medication disposal. Status: This process has been in place since June 2013. Anticipated Completion Date: As this is an ongoing process, no completion date can be given. Date Completed: See immediately previous response CAP Revision #1 - We will trial doing those audits weekly, to monitor the effectiveness, for one month. Additionally, there was some confusion as to stop dates vs expiration dates, which Ms Headstream and Ms. Somner were happy to address. Corrective Actions: See above. PRR ADC01466