Tucson Complex PPR ADC02791, October, AZ DOC, 2013
Download original document:
Document text
Document text
This text is machine-read, and may contain errors. Check the original document to verify accuracy.
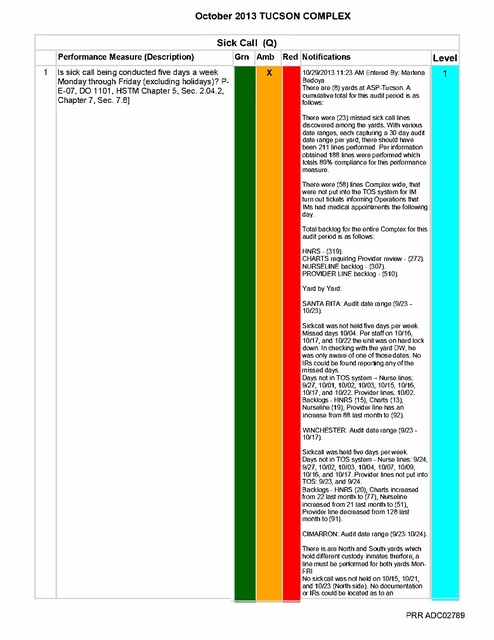
October 2013 TUCSON COMPLEX Sick Call (Q) Performance Measure (Description) Is sick call being conducted five days a week Monday through Friday (excluding holidays)? P E-07, DO 1101, HSTM Chapter 5, Sec. 2.04.2, Chapter 7, Sec. 7.6] Gm Amb Level Red Notifications 10/29/2013 11:23 AM Entered By: Marlena Bedoya There are (8) yards at ASP-Tucson. A cumulative total for this audit period is as follows: 1 There were (23) missed sick call lines discovered among the yards. With various date ranges, each capturing a 30 day audit date range per yard, there should have been 211 lines performed. Per information obtained 188 lines were performed which totals 89% compliance for this performance measure. There were (58) lines Complex wide, that were not put into the TOS system for IM turn out tickets informing Operations that IMs had medical appointments the following day. Total backlog for the entire Complex for this audit period is as follows: HNRS - (319). CHARTS requiring Provider review - (272). NURSELINE backlog - (307). PROVIDER LINE backlog - (510). Yard by Yard: SANTA RITA: Audit date range (9/2310/23). Sickcall was not held five days per week. Missed days 10/04. Per staff on 10/16, 10/17, and 10/22 the unit was on hard lock down. In checking with the yard OW, he was only aware of one of those dates. No IRs could be found reporting any of the missed days. Days not in TOS system - Nurse lines: 9127, 10/01, 10/02, 10/03, 10/15, 10/16, 10/17, and 10/22. Provider lines: 10/02. Backlogs - HNRS (15), Charis (13), Nurseline (19), Provider line has an increase from 88 last month to (92). WINCHESTER: Audit date range (9/23 10/17). Sickcall was held five days per week. Days not in TOS system - Nurse lines: 9/24, 9127, 10/02, 10/03, 10/04, 10/07, 10/09, 10/16, and 10/17. Provider lines not put into TOS: 9/23, and 9/24. Backlogs - HNRS (20), Charis increased from 22 last month to (77), Nurseline increased from 21 last month to (51), Provider line decreased from 128 last month to (91) CIMARRON Audit date range (9/23-10/24) There is are North and South yards which hold different custody inmates therfore; a line must be performed for both yards Mon FRI. No sickcall was not held on 10/15, 10/21, and 10/23 (North side) No documentation or IRs could be located as to an PRR ADC02789 October 2013 TUCSON COMPLEX Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 5 Are referrals to providers from sick call being seen within seven (7) days? [P-E-07] Level 1 Amber User: Marlena Bedoya Date: 10/29/2013 3:18:24 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.In-service all staff including providers on Sick Call 2.20.2.2 contract performance outcome 5 (Sick Call Attachment); Seen by Physician or Midlevel within 7 days a.Agenda/sign off sheet to verify 2.Monitoring (Sick Call Monitoring Tool) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties = FHA/DON/Medical Director/RDCQI/RVP Target Date- 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. PRR ADC02798 October 2013 TUCSON COMPLEX 3.Monitoring (UM Audit Tool) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties =ARMD/RDON/RVP/RDCQI/DON/ Target Date-11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 3 Is the utilization and availability of off-site services appropriate to meet medical, dental and mental health needs? [CC 2.20.2.3] Level 3 Amber User: Trudy Dumkrieger Date: 10/29/2013 1:30:45 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.Retrain FHA/DONs on ED management and expectations a.Agenda/sign off sheet to verify 2.Develop a site level process to assure, but not limited to: a.ED log completed and submitted daily to Regional office b.Access to custody transport logs c.Access to AIMS 3.Train site staff on ED management and expectations a.Agenda/sign off sheet to verify, inclusive of all pertinent staff 4.Review ED activity daily (in AM) with FHA/DON/MD (lead provider in absence of MD) to determine patient status and appropriate treatment plan a. Agenda/sign off sheet to verify, inclusive of all pertinent staff 5.Regional staff conduct weekly review of compliance to daily submission and appropriate patient disposition 6.Monitoring tool developed for self-monitoring and submission to site management and regional CQI 7.Initiation of monitoring tools at sites 8.Monitoring (UM Audit Tool) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties = VPO/ARMD/RDON/RVP/FHA/DON/MD/RDCQI Target Date- 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 10/11/13 Update – ED log sent to Regional office daily. PRR ADC02804 October 2013 TUCSON COMPLEX a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties = FHA/DON/IC/RDCQI/RVP Target Date-11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 10/11/13 Update – Statewide in Sept Redbook and MAR audit, results reviewed; to audit pharmacy in October related to Controlled Substances and Expired meds. PRR ADC02807 October 2013 TUCSON COMPLEX 4 Are inmates with a mental score of MH-3 and above seen by MH staff according to policy? [CC 2.20.2.10] Level 2 Red User: Jessica Raak Date: 10/29/2013 4:40:22 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1. Mental Health staff to receive education the importance of MH-3 inmates being seen according to policy. 2. Reinforce this in monthly staff meetings. 3. Continue to perform chart reviews to ensure inmates with an MH-3 score and above are being seen by Mental Health staff per policy. 4. Review treatment plans to ensuring that the IMs current MH score, according to the recognized system, is captured within the current treatment plan. Responsible Parties = MH Lead/RN/FHA/DON/MH Director/RCQI Target Date-11/30/13 5 Are inmates prescribed psychotropic meds seen by a Psychiatrist or Psychiatric Mid-level Provider at a minimum of every three (3) months (90 days)?[CC 2.20.2.10] Level 2 Red User: Jessica Raak Date: 10/29/2013 4:41:15 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.Monitoring (Mental Health Monitoring Tool) a.Audit tools developed b.Monthly site results discussed with RVP/MH Director c.Audit results discussed at monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties = RDCQI/RVP/MH Director/FHA/DON/MH Lead Target Date- 11/30/13 Continue to monitor monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 6 Are reentry/discharge plans established no later than 30 days prior release for all inmates with a MH score of MH-3 and above? [CC 2.20.2.10] Level 2 Red User: Jessica Raak Date: 10/29/2013 4:42:55 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.In-service staff on process expectations per Mental Health 2.20.2.10 contract performance outcome 7 (Mental Health Attachment) related to re-entry plan a.SMI patients will be followed by discharge planners utilizing the data from the SMI monthly report tool; MH3 patients will be given community resources by MH Clinicians and documented in the chart; all patients receiving psychotropic medications will be seen by Psychiatrist/Psychiatry CNP b.Agenda/sign off sheet to verify, inclusive of all pertinent staff 2.Monitoring (Mental Health Monitoring Tool) a.Audit tools developed b.Monthly site results discussed with RVP/MH Director c.Audit results discussed at monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Regional office for tracking and trending Responsible Parties = FHA/DON/Mental Health Director/RVP/RDON/RDCQI/MH Lead Target Date- 11/30/13 Continue to monitor monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. PRR ADC02814 October 2013 TUCSON COMPLEX Corrective Action Plans for PerformanceMeasure: Intake (Reception) 2 Has a Pano been completed? Alhambra, Perryville, Tucson Minors only [HSTM 2.9.2.6] Level 1 Amber User: Marlena Bedoya Date: 10/30/2013 11:02:08 AM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: Reinforce to staff that intake Pano to completed on all intakes. PRR ADC02818 October 2013 TUCSON COMPLEX Corrective Actions: Reinforce with staff the need to review medical records for contraindications when inmate has been placed in administrative segregation; document review in chart. Continue to monitor. PRR ADC02840 October 2013 TUCSON COMPLEX c.Audit results discussed a monthly CQI meeting. d.Minutes and audit reported monthly to Regional office for tracking and trending. Responsible Parties =FHA/DON/RDCQI/RVP/FHA Target Date- 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 6 Are there any unreasonable delays in inmate receiving prescribed medications? Level 2 Amber User: Trudy Dumkrieger Date: 10/29/2013 1:33:06 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by CorizonIntakes1.Standardized process for meds to be available to inmate upon transfer (Pharmacy Appendix 1 & 2) a.Intake Orders b.Private Prisons 2.In-service staff on process per PharmaCorr policy, a.Agenda/sign off sheet to verify, inclusive of all pertinent staff 3.Custody educated regarding contract requirements regarding inmate transfer with meds. 4.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsibile Parties = FHA/DON/Custody/RDCQI/RVP Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results 1.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending 2.Standardized process statewide to include, but not limited to (Appendix III.1.): a.Internal b.External 2.In-service staff on process and ADC policy titled “Continuity of Care Upon Transfer” Chapter 5, Section 5.0 (Appendices III.2.); a.Agenda/sign off sheet to verify, inclusive of all pertinent staff 3.Custody educated regarding contract requirements regarding inmate transfer with meds 4.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties = FHA/DON/Custody/RDCQI/RVP Target Date - 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 8 Are chronic condition medication expiration dates being reviewed prior to expiration to ensure continuity of care? [NCCHC Standard P-D-01] Level 2 Amber User: Trudy Dumkrieger Date: 10/17/2013 2:34:39 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.Standardized process for meds to be available to inmate upon transfer (Pharmacy Appendix 1 & 2) 2.In-service staff on process per PharmaCorr policy, a.Agenda/sign off sheet to verify, inclusive of all pertinent staff 3.Custody educated regarding contract requirements regarding inmate transfer with meds. 4.Monitoring (Appendix I. - IV Monitoring Tools) PRR ADC02854 October 2013 TUCSON COMPLEX a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsibile Parties = FHA/DON/Custody/RDCQI/RVP Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results 1.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending 2.Standardized process statewide to include, but not limited to (Appendix III.1.): a.Internal b.External 2.In-service staff on process and ADC policy titled “Continuity of Care Upon Transfer” Chapter 5, Section 5.0 (Appendices III.2.); a.Agenda/sign off sheet to verify, inclusive of all pertinent staff 3.Custody educated regarding contract requirements regarding inmate transfer with meds 4.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties = FHA/DON/Custody/RDCQI/RVP Target Date - 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 9 Are non-formulary requests being reviewed for approval or disapproval within 24 to 48 hours? Level 2 Amber User: Trudy Dumkrieger Date: 10/29/2013 1:34:02 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.Standardized process statewide, to include but not limited to (Pharmacy Appendix 1 & 2): a.Non-formulary process (Appendix I.1.d.) i.Reviewed for approval within 24-48 hrs ii.Providers notified decision within 24-48 hrs e.Manifest Reconciliation f.Inventory control g.Stock Medications h.Practitioner Cards (Appendis I.1.h.) i.Controlled Medications (Appendix I.1.i.) 2.In-service staff a.Using information from 8/19 - 11/13 Regional office mandatory in-service and PharmaCorr policy b.Agenda/sign off sheet to verify, inclusive of all pertinent staff (Appendix I.2.b.) 3.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties = FHA/DON/IC/RDCQI/RVP Target Date-11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 10/11/13 Update – Statewide in Sept Redbook and MAR audit, results reviewed; to audit pharmacy in October related to Controlled Substances and Expired meds. PRR ADC02855 October 2013 TUCSON COMPLEX 10 Are providers being notified of non-formulary decisions within 24 to 48 hours? Level 2 Amber User: Trudy Dumkrieger Date: 10/29/2013 1:34:30 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.Standardized process statewide, to include but not limited to (Pharmacy Appendix 1 & 2): a.Non-formulary process (Appendix I.1.d.) i.Reviewed for approval within 24-48 hrs ii.Providers notified decision within 24-48 hrs e.Manifest Reconciliation f.Inventory control g.Stock Medications h.Practitioner Cards (Appendis I.1.h.) i.Controlled Medications (Appendix I.1.i.) 2.In-service staff a.Using information from 8/19 - 11/13 Regional office mandatory in-service and PharmaCorr policy b.Agenda/sign off sheet to verify, inclusive of all pertinent staff (Appendix I.2.b.) 3.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed b.Weekly site results discussed with RVP c.Audit results discussed a monthly CQI meeting d.Minutes and audit reported monthly to Regional office for tracking and trending Responsible Parties = FHA/DON/IC/RDCQI/RVP Target Date-11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. 10/11/13 Update – Statewide in Sept Redbook and MAR audit, results reviewed; to audit pharmacy in October related to Controlled Substances and Expired meds. 11 Are medication error reports being completed and medication errors documented? Level 2 Amber User: Trudy Dumkrieger Date: 10/30/2013 3:24:49 PM Corrective Plan: See October action plan as submitted by Corizon. Corrective Actions: October Action plan submitted by Corizon1.Standardized process statewide to include, but not limited to : a.Medication error documentation/reporting (Pharmacy Appendix). 2.In-service staff on process and PharmaCorr policy. a.Agenda/sign off sheet to verify, inclusive of all pertinent staff. 3.Monitoring (Appendix I. - IV Monitoring Tools) a.Audit tools developed. b.Weekly site results discussed with RVP. c.Audit results discussed a monthly CQI meeting. d.Minutes and audit reported monthly to Regional office for tracking and trending. Responsible Parties =FHA/DON/RDCQI/RVP/FHA Target Date- 11/30/13 Continue to monitor weekly x 3 weeks, monthly until within compliance, then quarterly; monitoring frequency using audit tool per audit results. PRR ADC02856