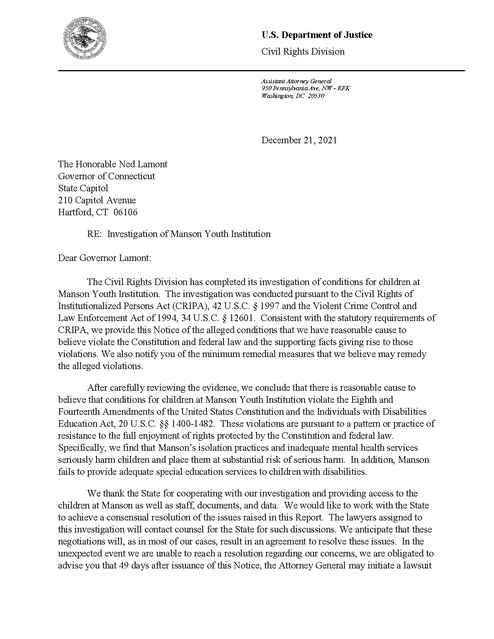
U.S. DOJ Investigation of Manson Youth Institution
Download original document:
Document text
Document text
This text is machine-read, and may contain errors. Check the original document to verify accuracy.
U.S. Department of Justice Civil Rights Division Assistant Attorney General 950 Pennsylvania Ave, NW - RFK Washington, DC 20530 December 21, 2021 The Honorable Ned Lamont Governor of Connecticut State Capitol 210 Capitol Avenue Hartford, CT 06106 RE: Investigation of Manson Youth Institution Dear Governor Lamont: The Civil Rights Division has completed its investigation of conditions for children at Manson Youth Institution. The investigation was conducted pursuant to the Civil Rights of Institutionalized Persons Act (CRIPA), 42 U.S.C. § 1997 and the Violent Crime Control and Law Enforcement Act of 1994, 34 U.S.C. § 12601. Consistent with the statutory requirements of CRIPA, we provide this Notice of the alleged conditions that we have reasonable cause to believe violate the Constitution and federal law and the supporting facts giving rise to those violations. We also notify you of the minimum remedial measures that we believe may remedy the alleged violations. After carefully reviewing the evidence, we conclude that there is reasonable cause to believe that conditions for children at Manson Youth Institution violate the Eighth and Fourteenth Amendments of the United States Constitution and the Individuals with Disabilities Education Act, 20 U.S.C. §§ 1400-1482. These violations are pursuant to a pattern or practice of resistance to the full enjoyment of rights protected by the Constitution and federal law. Specifically, we find that Manson’s isolation practices and inadequate mental health services seriously harm children and place them at substantial risk of serious harm. In addition, Manson fails to provide adequate special education services to children with disabilities. We thank the State for cooperating with our investigation and providing access to the children at Manson as well as staff, documents, and data. We would like to work with the State to achieve a consensual resolution of the issues raised in this Report. The lawyers assigned to this investigation will contact counsel for the State for such discussions. We anticipate that these negotiations will, as in most of our cases, result in an agreement to resolve these issues. In the unexpected event we are unable to reach a resolution regarding our concerns, we are obligated to advise you that 49 days after issuance of this Notice, the Attorney General may initiate a lawsuit under CRIPA to correct the alleged conditions we have identified if Manson officials have not satisfactorily addressed them. 42 U.S.C. § 1997b(a)(1). We hope, however, to resolve this matter through a cooperative approach and look forward to working with Manson leadership and staff to address the violations of law we have identified. Please also note that this Notice is a public document. It will be posted on the Civil Rights Division’s website. If you have any questions regarding this correspondence, please call Steven H. Rosenbaum, Chief of the Special Litigation Section, at (202) 616-3244. Sincerely, s/ Kristen Clarke Kristen Clarke Assistant Attorney General Civil Rights Division cc: William Tong Attorney General State of Connecticut Angel Quiros Commissioner Connecticut Department of Correction Derrick Molden Warden Manson Youth Institution Leonard C. Boyle Acting United States Attorney District of Connecticut Adrienne Mundy-Shephard Acting Director, Boston Office Office for Civil Rights U.S. Department of Education Attachment: Investigation of Manson Youth Institution INVESTIGATION OF MANSON YOUTH INSTITUTION United States Department of Justice Civil Rights Division December 21, 2021 TABLE OF CONTENTS I. INTRODUCTION ................................................................................................................. 1 II. INVESTIGATION................................................................................................................. 1 III. BACKGROUND ................................................................................................................... 2 IV. CONDITIONS IDENTIFIED................................................................................................ 2 A. B. C. V. Manson’s Isolation Practices Violate of the Constitution................................................... 3 1. Manson Routinely Isolates Children for Punishment ................................................ 4 2. Manson’s Isolation Practices Harm Children ............................................................ 7 Manson Fails to Provide Adequate Mental Health Services .............................................. 8 1. Manson Fails to Conduct Adequate Mental Health Assessments ............................. 9 2. Manson Fails to Provide Adequate Mental Health Care Treatment ........................ 13 Manson’s Provision of Special Education and Related Services Violates the Individuals with Disabilities Education Act ........................................................................................ 14 1. Manson Does Not Provide Children with Disabilities a Free Appropriate Public Education ................................................................................................................. 15 2. Manson Fails to Meet Its “Child Find” Obligations Under the IDEA..................... 22 MINIMAL REMEDIAL MEASURES................................................................................ 22 VI. CONCLUSION.................................................................................................................... 23 I. INTRODUCTION After an extensive investigation, the United States Department of Justice (DOJ) concludes that there is reasonable cause to believe that the conditions for children at the Manson Youth Institution (Manson) violate the Eighth and Fourteenth Amendments of the United States Constitution and the Individuals with Disabilities Education Act (IDEA), 20 U.S.C. §§ 14001482. These violations are pursuant to a pattern or practice of resistance to the full enjoyment of rights protected by the Constitution and federal law. Specifically, we find that Manson’s isolation practices and inadequate mental health services seriously harm children and place them at substantial risk of serious harm. In addition, Manson fails to provide adequate special education services to children with disabilities. The children housed at Manson are between the ages of 14 and 17. Most have significant histories of learning disabilities and mental illness. Yet they are deprived of the very services they need to navigate the correctional environment and develop skills and competencies to become productive, successful adults – and to which they are entitled under the law. When they misbehave, they are frequently subjected to harmful periods of disciplinary isolation, regardless of whether their conduct reflects typical adolescent behavior, whether it is a result of a failure to receive entitled services, or whether isolation will improve their behavior or facility security. In this report, we describe DOJ’s legal conclusions, the facts supporting those conclusions, and the minimum remedial measures necessary to address the identified violations. II. INVESTIGATION On October 15, 2019, the Department notified the State of its intent to conduct an investigation of conditions of confinement for children (i.e., youth under the age of 18) at Manson, pursuant to the Civil Rights of Institutionalized Persons Act, 42 U.S.C. § 1997 et seq. (CRIPA), and the Violent Crime Control and Law Enforcement Act of 1994, 34 U.S.C. § 12601 (Section 12601). The investigation focused on three issues: (1) whether Manson’s isolation practices violate the constitutional rights of children; (2) whether Manson’s mental health services for children are constitutionally inadequate; and (3) whether Manson violates the IDEA rights of children with disabilities. The Department conducted an onsite tour of Manson in January 2020. During this tour, Department attorneys and expert consultants conducted dozens of interviews of administrators and staff members, including security staff, counselors, mental health clinicians, teachers, administrators, as well as children confined at the facility. Additionally, Department attorneys and expert consultants reviewed over 31,000 pages of documents, including incident and use of force reports, policies and regulations, training materials, mental health records, education records, meeting minutes, lesson plans, shift rosters, unit logs, and investigative files. 1 Following the January 2020 tour, and throughout the pandemic, we continued to receive and review additional and updated documents and records from Manson. In February 2021, we conducted several additional interviews via videoconference. We appreciate the State’s cooperation and professionalism throughout the course of this investigation. Facility administrators and staff provided relevant documents and materials before, during and after our visit and facilitated our on-site visit as well as a number of videoconferences. III. BACKGROUND Manson is a State correctional facility operated by the Connecticut Department of Correction (DOC) which houses approximately 200 to 300 male youth under the age of 22 years, including children under the age of 18 (“children”) who have been transferred from juvenile court to the adult criminal court system. 1 Our investigation focuses exclusively on the children at Manson. During our investigation, Manson housed between 30 and 51 children. The majority of the children (approximately 75 to 80 percent) were being held pending trial and, therefore, had not been tried for (or convicted of) the crimes with which they were charged. Almost all of the children at Manson have at least one mental health diagnosis. Almost two-thirds have also been identified as eligible for special education services. The majority of children at Manson (approximately 75 to 85 percent) are identified as Black or Latinx. Manson’s under-eighteen population is housed separately from the older youth on two units, Units I and J. One wing within the J unit is used as an isolation unit. The individual cells on the isolation unit contain beds, and a sink/toilet. Children assigned to this unit are not permitted to keep personal possessions in their cells. IV. CONDITIONS IDENTIFIED We find that Connecticut is violating the constitutional and federal rights of children in three areas. First, Manson’s isolation practices harm children. Second, the State does not provide adequate mental health care to children. Third, qualified children with disabilities are not receiving the special education services to which they are entitled. 1 Under Connecticut law, children under the age of 18 who are charged with certain felonies are automatically transferred from juvenile court to the adult criminal court if the child was at least 15 years old when the alleged offense occurred. Conn. Gen. Stat. § 46b-127. Prosecutors may also petition the court to have children under 18 who are charged with certain lesser felonies transferred to adult criminal court if the child was at least 15 years old when the alleged offense occurred. Id. § 46b-127(b). 2 Ryan’s 2 experience illustrates many of the deficiencies we found in the conditions and care at Manson. Ryan was 15 years old when he was admitted to Manson as a pretrial detainee. His admission records include a diagnosis of Attention Deficit-Hyperactivity Disorder (ADHD) and a history of receiving special education services. His records also show he was exposed to a significant amount of violence and abuse as a child, including physical abuse by family members and a recent violent attack that left him with serious injuries. On a mental health screening administered upon intake at Manson, Ryan received high scores for anger, irritability, somatic complaints, thought disturbance, and trauma. None of this information was adequately explored by mental health staff in determining Ryan’s mental health needs. Instead, intake staff determined that he did not have any mental health issues that would require treatment. Several months later, Ryan was given diagnoses of conduct disorder, 3 ADHD, and marijuana abuse. Ryan’s school records show that, prior to admission to Manson, he was classified as “emotionally disturbed” and receiving 10 hours of special education services per week at his local school. But, based on Manson’s typical protocol, Manson’s educational team reduced Ryan’s special education services to just one hour per week, without any explanation of why a 96 percent reduction in services was justified, appropriate, or adequate. Throughout his time at Manson, Ryan exhibited numerous concerning behaviors, such as anger, irritability, anxiety, pressured speech, and mania, that may be symptoms of serious mental illness. Ryan regularly expressed not knowing how to cope with his feelings of anger. Ryan also reported trauma-related symptoms, for example, recurring nightmares about violence. Meanwhile, Ryan often got into trouble at Manson for infractions such as fighting, assaults, threats and “interfering with safety and security.” Sometimes, Ryan got in trouble at school. Other times, he got in trouble on his living unit. Frequently, he was punished with periods of time in disciplinary isolation, where his mental health deteriorated significantly. But there is little evidence in Ryan’s record that mental health staff explored whether his misbehaviors were symptoms of serious mental illness and/or trauma that required treatment as opposed to punishment, notwithstanding ample evidence suggesting that he was, indeed, experiencing a serious mental illness and trauma. Likewise, Manson failed to adequately explore whether Ryan’s special education services were sufficient to meet his needs and, if not, whether this deficiency was contributing to his classroom behavior. We found numerous cases like Ryan’s, where the deficiencies in Manson’s isolation practices, mental health services, and special education services harmed children in significant and cumulative ways. We discuss each deficiency below. A. Manson’s Isolation Practices Violate of the Constitution Manson imposes isolation on children as a disciplinary sanction for rule violations. Manson refers to this type of isolation as “Confined to Quarters” (CTQ). We find that Manson’s To protect the identities of the children at Manson, we have used pseudonyms based on the Social Security Administration’s list of most popular boys’ names for boys born in Connecticut in 2005. See Social Security Online, Popular Names by State, available at https://www.ssa.gov/cgi-bin/namesbystate.cgi. 3 “Conduct disorder” refers to a repetitive and persistent pattern of behavior in children involving difficulty following rules and societal norms. 2 3 CTQ practices subject children to significant harm in violation of the Constitution. See Farmer v. Brennan, 511 U.S. 825, 834 (1994). As noted, Manson houses children both pretrial and after conviction. Children at Manson post-conviction are protected under the Eighth Amendment, and children at Manson pretrial are protected under the Due Process Clause of the Fourteenth Amendment. City of Revere v. Mass. Gen. Hosp., 463 U.S. 239, 244 (1983); Bell v. Wolfish, 441 U.S. 520, 535 & n.16 (1979); Darnell v. Pineiro, 849 F.3d 17, 29 (2d Cir. 2017); Williams ex rel. V.W. v. Conway, 236 F. Supp. 3d 554, 582 & n.10 (N.D.N.Y. 2017). As pretrial detainees, the majority of children at Manson are subject to a more protective standard of liability under the Due Process Clause. Darnell, 849 F.3d at 35. We nevertheless apply the Eighth Amendment standard to conditions for all children at Manson because a pretrial detainee’s rights are “at least as great as the Eighth Amendment protections available to a convicted prisoner.” City of Revere, 463 U.S. at 244; see also Wolfish, 441 U.S. at 545 (pretrial detainees “retain at least those constitutional rights . . . enjoyed by convicted prisoners.”). The Eighth Amendment prohibits officials from subjecting anyone held in a correctional institution to “(1) a deprivation that is ‘objectively, sufficiently serious’ [as to deny] ‘the minimal civilized measure of life’s necessities,’ [with] (2) a ‘sufficiently culpable state of mind’ . . . such as deliberate indifference to inmate health or safety.’” Gaston v. Coughlin, 249 F.3d 156, 164 (2d Cir. 2001) (quoting Farmer, 511 U.S. at 834). Whether the harm is serious enough to establish a constitutional violation is “contextual and responsive to ‘contemporary standards of decency.’” Hudson v. McMillian, 503 U.S. 1, 9 (1992) (quoting Estelle v. Gamble, 429 U.S. 97, 103 (1976)). Establishing “deliberate indifference” under the Eighth Amendment requires showing that officials “know of, and disregard, an excessive risk to inmate health or safety.” Jabbar v. Fischer, 683 F.3d 54, 57 (2d Cir. 2012) (citing Farmer, 511 U.S. at 837). 4 “Evidence that a risk was ‘obvious or otherwise must have been known to a defendant’ may be sufficient for a fact finder to conclude that the defendant was actually aware of the risk.” Walker v. Schult, 717 F.3d 119, 125 (2d Cir. 2013). (quoting Brock v. Wright, 315 F.3d 158, 164 (2d Cir. 2003)). Additionally, courts may consider whether actions were “reasonably calculated to restore prison discipline and security,” Trammell v. Keane, 338 F.3d 155, 163 (2d Cir. 2003) (citing Hope v. Pelzer, 526 U.S. 730 (2002)). 1. Manson Routinely Isolates Children for Punishment DOC policy’s description of Manson’s disciplinary isolation program as “Confined to Quarters” obscures the harsh setting and conditions. Most of the children that we spoke with (as well as some staff) referred to CTQ as “the box.” When a child commits a rule infraction that security staff determines warrants assignment to CTQ, he is brought to the isolation unit in Cf. Darnell v. Pineiro, 849 F.3d 17, 35 (2d Cir. 2017) (finding, under a Fourteenth Amendment analysis, that pretrial detainees’ conditions of confinement violate the Due Process Clause where “the defendant-official acted intentionally to impose the alleged condition, or recklessly failed to act with reasonable care to mitigate the risk that the condition posed to the pretrial detainee even though the defendant-official knew, or should have known, that the condition posed an excessive risk to health or safety.”) (emphasis added). 4 4 handcuffs, strip searched for contraband, given a CTQ jumpsuit to wear, and placed alone in an empty cell without any personal property. Manson’s CTQ policy sets out a multi-step process where children must progress through four different CTQ levels (extended, high, moderate and low) before they are removed from CTQ status. Each of the four levels corresponds with a different degree of restrictiveness. Most children spend several days in isolation when sent to CTQ. On the highest CTQ levels (extended and high), children are locked in a bare cell on the isolation unit for a minimum of 23 hours a day. 5 Showers, phone calls and recreation must take place, if at all, during their one hour of out-of-cell time. 6 They are not allowed to attend school, religious services, or any other programming, and they eat their meals in their cells. Children remain on high CTQ until the unit manager authorizes transition to moderate CTQ. The timing of a child’s transition from high to moderate CTQ depends on the unit manager’s schedule. If the child is placed on high CTQ on a weekday, he typically will transition to moderate CTQ some time the following day. On weekends, the unit manager is not available and, therefore, the child must wait until the following Monday (or Tuesday, if Monday is a holiday) to transition to moderate CTQ. Children on moderate CTQ remain housed on Unit J’s isolation wing, continue to eat their meals in their cells and do not appear to attend programming. 7 They are, however, permitted to attend school on days it is in session. Thus, on weekdays, a child’s time in isolation is reduced by the number of hours he attends school. On the weekends (when school is not in session), there is no meaningful difference between high and moderate CTQ. 8 Manson sends children to CTQ on a routine basis and often for relatively minor offenses. Frequently, children at Manson are sent to CTQ for behaviors reflecting typical adolescent development, e.g., lower impulse control and self-regulation, poor decision-making, and higher Before 2019, extended CTQ was the default starting point for children assigned to CTQ for disciplinary isolation and, as the name suggests, involved a greater number of days in “the box.” Since early February 2019, Manson has not placed any children on extended CTQ. Children instead begin the disciplinary sanction on high CTQ. The only difference in restrictions between extended and high CTQ is that children on extended CTQ were required to wear handcuffs during their one hour of out-of-cell time and children on high CTQ are not. 6 Many of the children we interviewed reported that time out of cell was not always afforded, the actual duration was often shorter than one hour, there was not sufficient time to conduct all three activities, and that they did not engage in any large muscle activity during their time out of cell. In an attempt to verify, we reviewed a sample of “Out-ofCell Tracking Forms for Inmates on Sanctions,” on which staff are supposed to record “hour out” for all children in CTQ. We found that out-of-cell time was documented for only 67 percent of the sample we reviewed. Additionally, the Tracking Form does not indicate the duration of time out-of-cell or the child’s activities. 7 During interviews, Manson administrators were adamant that children on moderate CTQ attend programming. Yet every child we interviewed reported that they are not permitted to attend programming on moderate CTQ. To resolve this discrepancy, we reviewed a sample of Program Attendance Sheets for children who spent time in CTQ. However, the data was not available for every child in the sample, nor was it specific enough to verify attendance on the dates the children in the sample were in CTQ. Attempts to verify attendance in other programming likewise were unsuccessful due to missing documentation. 8 Once a child is moved to low CTQ, which is also called “loss of recreation,” he is returned to his general population unit. Children on low CTQ/loss of recreation participate in school and all programming except recreation. This loss of recreation time likely amounts to several hours of in-cell time on the weekdays and even more significant amounts of time on weekends (when school is not in session). 5 5 susceptibility to peer influence. Most of the time, nobody involved in the incident is injured. Even when children are calm and compliant, they are handcuffed, strip searched, and locked in isolation cells as punishment. Additionally, as previously noted, most of the children at Manson have mental health and other disabilities. As we discuss later in this report, the behaviors that give rise to punishment in CTQ are often related to unmet mental health and/or special education needs. Matthew’s case illustrates Manson’s use of disciplinary isolation as punishment for minor adolescent misbehaviors. Matthew was at school when he “repeatedly ignored several verbal directions to continue to complete the work he was provided” by his teacher. Manson staff responded by handcuffing him and taking him to the isolation wing where he was strip searched for contraband (none was found), given a CTQ jumpsuit to wear, and placed in a bare cell. Throughout this process, facility staff reported that Matthew was “calm and cooperative,” and “fully compliant” with staff’s directions. He nonetheless received a disciplinary report for “flagrant disobedience” and spent one day on high CTQ and three days on moderate CTQ. In another example, Michael was in class when his teacher had to redirect him for opening an absent teacher’s desk drawer. When the teacher left the room briefly, Michael reopened the drawer, took out a marker and began drawing on his shoes. In her report, the teacher notes that she had to ask Michael to put the marker away three more times before he complied. Michael was cited for “interfering with safety and security” and, in the order imposing CTQ, corrections staff states that Michael’s “continued presence in the general population poses a serious threat to life, property, self, other inmates and/or the security of the facility.” Michael was handcuffed, strip searched for contraband (none was found), given a CTQ jumpsuit to wear, and placed in a bare cell on the isolation wing. For his offense, Michael spent four days on extended CTQ. Nicholas spent three days on high and another four on moderate CTQ after being cited for “flagrant disobedience” in the classroom. According to the incident report, Nicholas refused to follow his teacher’s directions and used profanity. As with the others, Nicholas was “compliant” when he was handcuffed, strip searched for contraband (none was found), and locked in a bare cell. We found numerous other examples of children being isolated in CTQ as punishment for rule infractions involving such misbehaviors as: • • • Knocking workbooks to the floor in school (resulting in two children receiving one day high CTQ and three days moderate CTQ). Both children later reported that they were just “messing around,” and the two were friends. Notably, the responding officer reported that he had to ask why the teacher called for assistance because he was observing a “calm classroom.” Using vulgar language, yelling, and failing to comply with verbal directions (resulting in one day on high CTQ and three days on moderate CTQ). “Refusing housing” (resulting in one day on high CTQ and one day medium CTQ). The child had informed nurses that he did not feel safe on his unit and had been threatened with assault, but he would not say who made the threats. Because he would not return to 6 • his unit, he was handcuffed, strip searched for contraband (none was found), given a CTQ jumpsuit to wear, and placed in a bare cell. Speaking extremely loudly and using disrespectful words in an aggressive manner to his teacher and responding officers (resulting in three days on high CTQ and three days on moderate CTQ). 9 2. Manson’s Isolation Practices Harm Children Isolation places children at significant risk of harm. V.W. v. Conway, 236 F. Supp. 3d 554, 583 (N.D.N.Y. 2017) (enjoining the disciplinary isolation of children in an adult facility as violative of the Eighth Amendment). 10 Because of their developmental immaturity, brain development, and lack of effective coping mechanisms, children are uniquely vulnerable to the serious and lasting damage isolation causes. 11 In addition to exacerbating existing mental health conditions, isolation can cause a host of other harms to children, including stress-related reactions, sleep disturbances, anxiety, aggression, cognitive dysfunction, self-harming behavior, and suicide. Children at Manson suffer serious harm as a result of Manson’s isolation practices. For example, Ryan (discussed above) experienced serious deteriorations of his mental status while in CTQ. In an interview, Ryan described experiences of hearing people who were not there and that these experiences would worsen when he was in CTQ. He described “seeing things” and being frightened in CTQ, such as toilets flushing on their own and lights going on and off by themselves. In spite of serious deteriorations of his mental health while on CTQ, Ryan was placed there repeatedly, including, in at least one instance, immediately after being released from suicide watch. The child who received this sanction is Ryan, whose many symptoms of a serious mental illness were not adequately assessed and whose special education services were drastically cut (discussed at the beginning of this Report). 10 The V.W. court considered expert testimony describing how isolation “perpetuates, worsens, or even in some cases precipitates mental health concerns that can lead to long-term and often permanent changes in adolescent brain development.” Id. at 570-71. In enjoining defendants’ use of disciplinary isolation on children, the court relied on the “broad consensus among the scientific and professional community that juveniles are psychologically more vulnerable than adults.” Id. at 583; see also Paykina ex rel. E.L. v. Lewin, 387 F. Supp. 3d 225, 243 (N.D.N.Y. 2019) (enjoining adult correctional facility from isolating a child and noting that “the deleterious effects of solitary confinement on mentally ill juveniles are a matter of common knowledge in the medical and psychiatric communities”); A.T. v. Harder, 298 F. Supp. 3d 391, 416 (N.D.N.Y. 2018) (granting preliminary injunction to plaintiff class of children in an adult facility, finding “plaintiffs are substantially likely to succeed on their claim that the [adult jail’s] widespread, excessive usage of solitary confinement on juveniles is unconstitutional.”); Doe v. Hommrich, No. 3-16-0799, 2017 WL 1091864, at *2 (M.D. Tenn. Mar. 22, 2017) (enjoining the use of disciplinary isolation of children because the practice likely constitutes “inhumane treatment” in violation of the Eighth and Fourteenth Amendments). 11 See, e.g., Nat’l Comm’n on Correctional Health Care, Position Statement on Solitary Confinement 2 (Apr. 2016) (Because children’s brains are still developing, the “developmental, psychological, and physical damage [is] more comprehensive and lasting.”). 9 7 Other children similarly experienced deteriorations in their mental health while on CTQ, including having suicidal thoughts. When Anthony was placed in CTQ, he reported that his thoughts were racing and evidenced an inability to think straight. He reported that he “can’t be locked in a room like that” and that he had been thinking about killing himself. When Joshua was placed in CTQ, he tied a sheet to his bed and said that he “think[s] about suicide a lot.” He stated that he was stressed out and felt unable to “do this” anymore and reported he would be less stressed if he were out of CTQ. Not only is isolation harmful to children, but “research shows that isolation is an ineffective disciplinary technique for restoring facility security and is in fact counterproductive to facility discipline and security.” V.W., 236 F. Supp. 3d at 568 (granting preliminary injunction prohibiting disciplinary isolation of children in an adult facility as violative of the Eighth Amendment). Effective strategies for increasing safety and reducing violence among adolescents rely on reducing idle time and increasing structured activities led by an adult – not increasing idle time and reducing structured activities led by an adult. Thus, Manson’s isolation practices do not serve a legitimate government purpose and show a deliberate indifference to the growing body of evidence that isolation is particularly harmful to children. See Bell v. Wolfish, 441 U.S. 520, 538-39 (1979); Farmer, 511 U.S. at 834-35. 12 B. Manson Fails to Provide Adequate Mental Health Services Manson fails to provide children with adequate mental health supports and services. The Constitution requires that Manson provide children with adequate treatment for serious medical needs, including serious mental health needs. Langley v. Coughlin, 888 F.2d 252, 254 (2d Cir. 1989); Davis v. McCready, 283 F. Supp. 3d 108, 116 (S.D.N.Y. 2017). Mental health treatment is an “integral part of medical care,” and “the basic legal principle is clear and well established . . . that when incarceration deprives a person of reasonably necessary medical care (including psychiatric or mental health care) . . ., the prison authorities must provide such surrogate care.” Langley v. Coughlin, 888 F.2d at 254. As with excessive isolation, deprivations of mental health care violate the Eighth Amendment if they are sufficiently serious and the prison official is deliberately indifferent to prisoner health or safety. 13 Smith v. Carpenter, 316 F.3d 178, 186 (2d Cir. 2003); Salahuddin, 467 F.3d at 279-81. Several deficiencies in care may collectively amount to a constitutional violation “when they have a mutually enforcing effect that produces the deprivation of a single, identifiable human need. . . .” Wilson v. Seiter, 501 U.S. 294, 304 (1991). Officials act with deliberate indifference if they know that failing to provide adequate mental health care will pose a substantial risk of serious harm. A “factfinder may conclude that a Manson previously also isolated children for extended periods of time in its “Security Risk Group” program, which is a DOC-wide program intended to address gang activity in Connecticut’s prisons. In 2019, Manson stopped applying the SRG policy, as written, to children and now houses children who have been designated SRG with the general population. 13 As above, we apply Eighth Amendment standard to both pretrial detainees and convicted children because a pretrial detainee’s rights are “at least as great as the Eighth Amendment protections available to a convicted prisoner,” City of Revere, 463 U.S. at 244. However, we note that most of the children at Manson are subject to the Due Process Clause’s more protective standard. Darnell v. Pineiro, 849 F.3d 17, 35 (2d Cir. 2017). 12 8 prison official knew of a substantial risk from the very fact that the risk was obvious.” Farmer, 511 U.S. at 842. Inadequate mental health care poses a particularly high risk of serious harm to children because (as previously discussed) they are more psychologically vulnerable than adults and are more likely to suffer long-term or permanent psychological damage. A.T. v. Harder, 298 F. Supp. 3d 391, 414 (N.D.N.Y. 2018) (citing Graham v. Florida, 560 U.S. 48, 68 (2010); Roper v. Simmons, 543 U.S. 551, 569 (2005)). 1. Manson Fails to Conduct Adequate Mental Health Assessments Manson’s mental health staff regularly fail to consider relevant information available -through records, screening tools, and interviews -- when assessing a child’s mental health needs. Instead, children are assigned behavioral diagnoses and given treatment plans focused on adjusting to prison life, regardless of how a child’s mental health may impact his ability to function at Manson. In particular, staff frequently ignore or downplay evidence of past trauma, as well as the relationship between substance abuse and other psychiatric disorders. As a result, children at Manson suffer the debilitating effects of untreated mental illness. Many children are also subjected to harmful isolation as punishment for behaviors that are symptoms of their untreated mental illness. a. Manson’s Intake Assessments Are Inadequate When a child arrives at Manson, a clinical staff member conducts an initial mental health assessment. Based on this assessment, the clinician assigns the child a mental health status score ranging from one to five. A score of one or two reportedly indicates that the child is not in need of mental health treatment. Children who score a three or four reportedly are offered some level of mental health treatment. Children who score a five reportedly are placed in the infirmary. Approximately 40 percent of incoming children are identified at intake as needing mental health treatment. However, this percentage rises significantly after admission. Thus, at the time of our January 2020 onsite visit, 64 percent of the total population of children at Manson were identified as in need of mental health treatment. This sharp rise in the mental health caseload after intake suggests that initial assessments are not identifying all incoming children with mental health needs. Our review of individual cases confirms this is so. 14 Important information frequently is ignored during the initial intake assessment. For example, Jack was 16 years old when he was admitted to Manson. His record indicates that he suffered a serious head injury as a young child and was previously identified as having an IQ of 62. His record also notes possible lead poisoning, a psychiatric hospitalization at age nine, and a long history of school suspensions for fighting. Notwithstanding that these are all indicators of intellectual and other cognitive deficits, Jack was given diagnoses of conduct disorder and “disruptive mood,” and a treatment plan focused on offering him structure and helping him make better choices. Mental health staff generally attribute this rise in the number of children needing mental health services to them becoming more aware of the severity of their criminal case status and then becoming emotionally distraught. Our review of individual cases, however, indicates otherwise. 14 9 During his time at Manson, Jack repeatedly was sent to CTQ for behaviors that are symptoms of intellectual or other cognitive deficits, such as mood instability and ongoing irritability. Yet mental health staff failed to adequately explore how Jack’s reported brain injury and extremely low IQ might impact his ability to function at Manson. Even when additional testing provided more evidence of cognitive deficits and therapeutic interventions (e.g., medication) were clearly not working, mental health staff still failed to question the working diagnosis and consider other possible explanations for his difficulties. b. Manson Fails to Adequately Identify and Assess Signs of Trauma Mental health assessments conducted at Manson repeatedly miss or minimize the significance of a history of exposure to severely traumatic events, as well as the resultant mental health difficulties and impact on the child’s ability to function. In fact, only three children had a diagnosis of posttraumatic stress disorder (PTSD) at the time of our onsite visit, while approximately two-thirds had a diagnosis of conduct disorder and two-thirds were diagnosed with a marijuana-related disorder. 15 As a result of failing to consider trauma, children with trauma-related mental health issues continue to suffer. Additionally, many children with such untreated mental health needs end up exhibiting related behaviors for which they subsequently are punished. A history of repeated exposure to traumatic events, or one extremely traumatic event, is very common in the population of children housed at Manson and can have significant negative effects on mental health. Children who have been exposed to violent trauma may develop neurological difficulties, trauma-specific psychological difficulties, developmental difficulties, and other associated functional difficulties. Each of these categories of symptoms cause children significant emotional distress and impair their ability to function, and the symptoms are mutually exacerbating. Many children at Manson have clear indicators of trauma in their records that Manson fails to consider adequately when assessing their mental health needs. For example, Tyler was 16 years old when he was admitted to Manson. His record reflects he was raised by his grandmother and that, prior to age 15, had no history of significant mental health issues or behavior problems other than some marijuana and alcohol use. When he was 15, his grandmother died and his behavior deteriorated. At Manson, Tyler was given diagnoses of conduct disorder and marijuana abuse, and a mental health score of one (indicating he was not in need of mental health services). During his time at Manson, Tyler frequently was charged with rule infractions such as fighting, threatening staff, and “interfering with safety and security,” and punished with many days in disciplinary isolation as a result. After nearly a year, he made a self-referral for a mental health sick call, during which he reported to the clinician that he had experienced many traumatic events. He became anxious and teary as he talked about his grandmother’s death. He also described repeated exposure to community violence, including witnessing a beheading when he was twelve years old. He reported recurring visions about the beheading and expressed that he The diagnostic records of three additional children noted, “rule out PSTD,” meaning they might have PTSD but the clinician was not certain. 15 10 did not believe his life would be very long. His clinician noted that Tyler was not suffering from “full PTSD” (meaning he did not exhibit all of the symptoms necessary to make a definitive diagnosis of PTSD), but the clinician did not adequately follow up to determine whether Tyler exhibited additional symptoms that he had not volunteered and would not know were important to mention for diagnostic purposes. Instead, she continued the diagnosis of conduct disorder. Benjamin was 16 years old at the time of his admission to Manson. During his initial mental health assessment, he revealed that he had “lost some friends and family,” and he scored high on screening tool measures for anger and irritability. When interviewed by our mental health consultant, Benjamin freely shared that four of his friends had been killed; one friend was stabbed and the other three were shot. Benjamin also explained that since his friends were murdered, he has been “quick to snap” and when that happens it takes a long time for him to calm down. But there is no evidence that mental health staff conducted any exploration of Benjamin’s trauma history and how it may be causing Benjamin’s difficulties in controlling his temper. Instead, Benjamin was diagnosed with conduct disorder, moderate intellectual disability, and attention deficit hyperactivity disorder, and given treatment plan goals of improving his coping skills and learning to follow orders. 16 Manson failed to assess Benjamin’s mental health needs not only at intake but at various later points. For example, at one point, Benjamin shared with his clinician that he was writing a song about his four deceased friends. There is no evidence that his clinician followed up to explore the impact these sudden, violent deaths had on Benjamin, and his diagnoses and treatment plan remained unchanged. Joseph exhibited several indicators of past trauma that should have been considered in determining a diagnosis and treatment plan. For example, on a screening tool administered during his initial assessment, Joseph indicated “bad or terrifying things have happened to me” and having been “badly hurt or at risk of being badly hurt.” Although these responses suggest a history of trauma, this wasn’t explored by mental health staff. Other behaviors that were subsequently noted likewise were never identified as potential indicators of trauma, such as hypervigilance, over-reactivity and episodes of dissociation when he is threatened with being hit. Instead, he was given a diagnosis of anti-social personality disorder. Christopher reported during his initial mental health assessment that he had been stabbed and then hospitalized for five days with a chest tube. At intake, he also reported having nightmares about being stabbed. But these indicators of trauma were not explored to determine whether, and to what extent, they may impact Christopher’s mental health. Instead, he was diagnosed as “oppositional/defiant,” and given a mental health score of two (meaning he was not in need of mental health services). When interviewed by our mental health consultant, Daniel shared that his brother had been shot and killed. He described how he deteriorated following that incident. None of this history nor his trauma-related symptoms was uncovered during his mental health assessment and Benjamin’s record also indicated that he had an IQ of 40 and a history of receiving special education services. As with Jack, mental health staff failed to consider how Benjamin’s reported intellectual disability might impact his ability to function at Manson. 16 11 he was not given a trauma-related diagnosis. Instead, he was given a diagnosis of conduct disorder and assigned a mental health score of two. c. Manson Fails to Adequately Assess and Treat Children with Dual Diagnoses of Substance Abuse and Other Psychiatric Disorders Manson also fails to adequately assess and treat children with dual diagnoses of substance abuse and some other psychiatric disorder. As noted above, about two-thirds of the children at Manson are given a marijuana-related diagnosis in addition to other psychiatric disorders. Treatment of individuals with dual diagnoses of substance abuse and some other psychiatric disorder must involve an integration of the treatments for both disorders. In the absence of such integrated treatment, neither their substance abuse nor the other mental health difficulties will be addressed in a meaningful way. Yet there is very little exploration at Manson about the circumstances of children’s marijuana use or consideration of the implications of dual-diagnoses for treatment. The minimization of the significance of marijuana use, the lack of exploration of why a child may have started abusing marijuana, and the failure to recognize the possible relationship between marijuana use and other mental health difficulties can be extremely harmful. If the possibility that marijuana use is self-medication for other mental health difficulties is not even considered, the diagnosis of other mental health difficulties may be missed. Additionally, if a child’s behavior deteriorates because he is unable to self-medicate at Manson, his behavior will be inaccurately viewed as a behavioral problem, exposing the child to punishment in CTQ. d. Manson Fails to Adequately Assess Children Placed in CTQ Children at Manson are not adequately assessed by mental health staff prior to placement in CTQ. As a result, children are punished with time in isolation for behaviors resulting from unmet mental health needs. And, as discussed earlier, isolation serves to worsen children’s mental health symptoms. Manson’s mental health policies and procedures require mental health staff to assess a child when disciplinary charges are filed if he has a mental health score of four or five or if security staff request an assessment. However, the purpose of this assessment is limited to identifying those children who are so severely ill that they have to be placed in the infirmary, and clearing the rest for placement in CTQ. Manson does not assess whether the problematic behavior is symptomatic of a mental health issue that requires mental health intervention (as opposed to misconduct that requires discipline). Nor does Manson assess the capacity of the child to cope with and benefit from the discipline. As we discussed above with respect to Ryan’s experience, Manson’s mental health staff do not consider to what extent the charged behavior might have been a product of mental health issues nor whether mental health treatment might be a more appropriate intervention. Even for children such as Christopher, whose symptoms of trauma were previously discussed and who was frequently sent to CTQ for various infractions, Manson failed to adequately consider whether his behavior was a symptom of an unmet mental health need. Paykina, 387 F. Supp. 3d at 244 (“accumulating disciplinary violations” is evidence of deteriorating mental health). 12 In addition, subjecting children who experience trauma-related mental health difficulties to isolation provides more opportunity to focus on the traumas endured, which may exacerbate their symptoms. For example, Ethan was frequently placed in CTQ. Each time, his nightmares, flashbacks and episodes of dissociation (all symptoms of his trauma-related mental health difficulties) increased. See Paykina, 387 F. Supp. 3d at 239 (children “are particularly susceptible to worsening mental health problems as a result of solitary confinement because ‘juvenile brains are continuing to develop’”). 2. Manson Fails to Provide Adequate Mental Health Care Treatment Manson fails to provide adequate treatment to children with serious mental illness in several important aspects. First, as already discussed, when assessments are inaccurate, then individual treatment plans will not address the child’s mental health needs. Additionally, Manson’s practice of reducing a child’s mental health score when he refuses the treatment offered is highly inappropriate. Finally, group counseling programs available at Manson are designed primarily for adults and of little therapeutic value to children. a. Manson Inappropriately Reduces Mental Health Scores and Services When Children Refuse the Treatment Offered When a child refuses to participate in individual therapy or does not comply with the prescribed medication regimen, the mental health staff does not attempt to develop a plan to try to keep the child engaged in therapy or obtain medication compliance. Instead, Manson reduces the child’s mental health score to two and discontinues mental health services. While it can be difficult to engage a child in therapy, the practice of reducing his mental health score based on non-compliance is not appropriate. Such a response not only erroneously blames the child for his failure to engage in therapy (when more likely, the focus of therapy is non-responsive to his needs for the reasons discussed above), but it denies the child access to treatment even though he has been identified as in need of treatment. Moreover, if that child subsequently commits a rule infraction due to his unmet mental health needs, he will be sent to CTQ as punishment. And because his mental health score is two, he will not even be assessed prior to placement in CTQ unless security staff requests it – even though he has a documented mental health need. For children whose medications are discontinued due to non-compliance, the risk of harm likewise is very significant. Sometimes, a child’s mental health can deteriorate quite obviously and significantly after medication is discontinued. For example, James ended up on suicide watch after discontinuation of psychiatric medication. In another case, Alexander became psychotic following discontinuation of medication. b. Manson’s Group Therapy Services Are Not Appropriate for Children Finally, group therapies are generally oriented towards the adult population and of little value to the children at Manson. In fact, the most common reason noted in mental health records for finding that a child is not appropriate for a given group is that the child is not mature enough 13 to engage in the therapeutic work of the group. We found no therapy groups that are specifically designed for the younger population, nor any groups whose membership is limited to children. In addition, the available groups are all short-term (i.e., 8 to 12 weeks), which is not suitable for children. For example, the trauma group runs for about eight weeks, and virtually all of the participants are age 18 or older. Children with trauma-related mental health difficulties process issues differently than adults, and need a much longer period of time to benefit from a trauma-informed group therapy program. Thus, even if a child with trauma-related mental health needs was placed in this group, he is not likely to benefit from the experience. Similarly, as noted above, for many of the children at Manson, their history of substance abuse is very much tied to other mental health difficulties. The available substance abuse group therapy programs (i.e., the drug education and smart recovery groups) are not designed to address dually-diagnosed children. Given the short duration of these programs and the fact that the participants in the substance abuse group programs are primarily age eighteen or older, the existing programs are not appropriate even for children who have only a substance abuse disorder. Not surprisingly, mental health staff acknowledge that the available substance abuserelated groups are ineffective for the overwhelming majority of the children at Manson. C. Manson’s Provision of Special Education and Related Services Violates the Individuals with Disabilities Education Act Congress enacted the Individuals with Disabilities Education Act (IDEA) to ensure that children with disabilities have access to a “free appropriate public education that emphasizes special education and related services designed to meet their unique needs.” 20 U.S.C. §§ 1400(d)(1)(A) and 1412(a)(1)(A). Children with disabilities in correctional facilities do not forfeit their right to special education services. 17 Instead, the IDEA explicitly applies to “adult correctional facilities” that “are involved in the education of children with disabilities.” 34 C.F.R. § 300.2(b)(1)(iv). Educational services at Manson, including special education services, are provided by Unified School District #1 (USD #1), the school district that provides educational services to individuals incarcerated in DOC facilities. The DOC Commissioner serves as the Chairperson of the USD #1 school board, and the Superintendent of Schools administers and supervises the daily operations of the school district. The school at Manson has its own administrative team, led by a school principal. Nearly all of the children at Manson are enrolled in the High School Program, which includes a curriculum of English, math, science, social studies, and physical education. Over 60 percent of the children enrolled in the High School Program are eligible for special education services. With specific and very limited exceptions, age-eligible students with disabilities in adult prisons are entitled to a free appropriate public education under the IDEA. 34 C.F.R. §§ 300.101-102, § 300.324 (d)(1)(i). 17 14 1. Manson Does Not Provide Children with Disabilities a Free Appropriate Public Education Manson fails to provide special education and related services that enable the children to access appropriate educational services that are particularized to their needs and abilities, as required by the IDEA. a. Manson Routinely Reduces Special Education Services without Consideration of Individualized Needs Children with disabilities are entitled to a free appropriate public education in conformity with an individualized education program (IEP). 18 Instead of tailoring each IEP to the unique needs of each particular child, Manson uniformly reduces the special education services provided to all the children who enter the facility. No matter the child’s “present levels of achievement, disability, and potential for growth,” Endrew F., 137 S. Ct. at 999, the children’s special education services are consistently, and often dramatically, reduced without any explanation or justification documented in the students’ IEPs. For example, Christopher has a diagnosis of ADHD. In his local school district, Christopher was receiving special education services for 11 hours per week. Upon admission to Manson, Christopher’s special education services were reduced by over 90 percent – to just one hour per week – without justification. Even when his Manson teachers subsequently noted that Christopher’s “effort and work production were inconsistent across all content areas,” that he was failing two subjects due to a “refusal to complete assigned work,” and “ha[d] received both formal and informal disciplinary reports,” Manson did not adjust or increase his special education service hours. Similarly, Manson reduced special education services for David, a student classified as having an “other health impairment,” 19 by over 90 percent. David’s service hours were reduced from 23 hours per week in his local school district to only 30 minutes per week at Manson despite that his IEP from his local school district noted “comprehension difficulties,” “weaknesses in basic writing skills,” “difficulty with attention,” and “weaknesses in basic mathematical concepts,” including weaknesses that required “specialized instruction.” His prior IEP also noted that David had “difficulty managing distractions and requires a self-contained behavioral program” and that his “difficulties sustaining attention, understanding and 34 C.F.R. § 300.17(d). See also R.E. v. New York City Dep’t of Educ., 694 F.3d 167, 175 (2d Cir. 2012) (“To ensure that qualifying children receive a [free appropriate public education], a school district must create an individualized education program (‘IEP’) for each such child.”). A child’s IEP must be tailored to the unique needs of a particular child. Endrew F. v. Douglas Cty. Sch. Dist., 137 S. Ct. 988, 1000 (2017). The Supreme Court has recognized that “[a]n IEP is not a form document. It is constructed only after careful consideration of the child’s present levels of achievement, disability, and potential for growth.” Id. at 999. See also id. at 994 (the procedures for drafting an IEP “emphasize collaboration among parents and educators and require careful consideration of the child’s individual circumstances.”). 19 “Other health impairment means having limited strength, vitality, or alertness, including a heightened alertness to environmental stimuli, that results in limited alertness with respect to the educational environment.” 34 C.F.R. § 300.8(c)(9). 18 15 communicating his feelings, and low frustration level limits his access [to] the general education environment.” As discussed at the beginning of this Report, Manson also reduced special education services for Ryan, a student classified as emotionally disturbed from 10 hours per week in his local school district to one hour per week at Manson. Manson inexplicably continued to provide only these reduced services to Ryan even though a subsequent IEP at Manson recognized that he would benefit from a specialized program, noting that “[d]ue to Ryan’s mood dysregulation, anger control, executive functioning, and limited self-esteem, he may benefit from a specialized program to be successful in the general curriculum,” and, similarly, that “[d]ue to Ryan’s deficits in how he processes and reasons verbal information, he may require a specialized program.” On average, the IEPs of children at Manson provided just over one hour per week of special education services at Manson, as compared with nearly 18 hours of services per week in the IEPs created by their local school districts. When asked about the reduction in services, one educational administrator indicated that, under the students’ prior IEPs, the students “still ended up in prison,” so the school district is “trying another route.” IEP Special Education Services (hours per week) 20 15 10 5 0 Manson Home School District Manson reduces services in spite of the fact that the teams creating the IEPs in the local school district generally had a more extensive knowledge and background about the students and their individualized needs than the Manson educational staff because the local school districts typically had worked with the student over much longer periods of time. For example, shortly after Thomas was incarcerated at Manson, his home school district reviewed and updated his IEP. 20 Thomas had been a student in his local high school for more than a full school year, giving the school district an opportunity to get to know Thomas and the supports and interventions he required. Thomas was classified as having an “other health impairment, ADD/ADHD,” and his local school district IEP notes that “Thomas has significant delays in attention and listening skills and requires an individualized program in an environment that can provide structure and added accommodations in order to academically progress.” The IEP also 20 Thomas’ local school district scheduled the meeting to determine whether Thomas’ arrest was a manifestation of his disability. As described below, before a school can change the placement of a child with a disability, it must conduct a “manifestation determination” to determine if the questioned behavior was caused by, or had a direct and substantial relationship to, the child’s disability or the failure to implement the child’s IEP. 20 U.S.C. § 1415(k)(1)(E). 16 notes that “Thomas’ difficulties with controlling impulses and aggression and his inability to follow through on tasks and directions interfere with his peer and adult relationships and his ability to function independently in the classroom. He requires a high degree of adult support to help him gain control.” In the IEP, the local school district indicated that Thomas should receive 27.5 hours of special education services per week that were to be provided with a special education teacher in a separate resource or related services room (not the regular classroom). Although his home school district determined that Thomas needed a high level of intensive services and interventions, Manson’s IEP, written about two weeks after the local school district’s IEP and just three weeks after Thomas arrived at Manson, reduced his special education services to less than two hours per week. At the meeting at Manson where this new IEP was reviewed and adopted, there was no discussion of why services were reduced or how these reduced services would meet Thomas’ individual educational needs. The students at Manson described how the reductions in services impacted their ability to function in Manson’s classrooms. Dylan described being in a special education classroom all day with five to eight other students in his local school district, then transitioning to Manson where he saw his special education teacher one hour per week. The student noted that he frequently got into trouble in the regular education classroom at Manson and wished that he could have more one-on-one attention in school at Manson. Significantly, we were unable to verify the extent to which students receive even these reduced services. Manson had no standardized system to document whether and when special education and related services were provided, relying instead on individual special education teachers and school psychologist to develop and maintain their own tracking systems, without any oversight from the school or school district to ensure that services are provided in accordance with each student’s IEP. Additionally, Manson’s limited instructional time further reduces the special education and related services that students receive. Classes in Manson’s high school program frequently were canceled due to teacher absences, facility or unit lockdowns, and trainings and other events. Even when classes are not canceled, students rarely attend school for the full five hours scheduled each day (three hours in the morning and two hours in the afternoon). Both morning and afternoon classes typically commenced 20 to 30 minutes after their scheduled start time due to delays in children being escorted from their living units to the school. On average, students miss about 15 percent of their scheduled instructional time each day. This loss of instructional time significantly reduces the special education services the students receive, particularly when students are scheduled to receive services during a class period that starts 30 minutes late. b. Manson Routinely Fails to Implement the Modifications and Accommodations Required by IEPs To ensure that children with disabilities can access the general curriculum, the IDEA requires that school districts “adapt[], as appropriate to the needs of an eligible child under this part, the content, methodology, or delivery of instruction.” 34 C.F.R. § 300.39(b)(3). Although IEPs developed by Manson list modifications and accommodations designed to ensure access to 17 the general curriculum, 21 the modifications and accommodations consistently are not provided in the general education classrooms. The regular education teachers are responsible for implementing modifications and accommodations in the classroom, most often without the support of a special education teacher. This is especially challenging at Manson because of the high percentage of children who are eligible for special education services. 22 The general education teachers receive no training on how to implement modifications and accommodations in their classrooms or provide individualized instruction, and Manson relies on individual regular education teachers to look at each student’s file to identify the modifications and accommodations required by each student’s IEP. c. Manson Routinely Fails to Provide the Related Services Required by Children’s IEPs Manson fails to adequately provide the related services required by the IDEA. Related services are “developmental, corrective, and other supportive services . . . as may be required to assist a child with a disability to benefit from special education.” 20 U.S.C. §1401(26)(A). These services include “speech-language pathology,” “psychological services,” “physical and occupational therapy,” “counseling services,” and “medical services.” Id. Manson automatically reduces the “related service” of counseling in students’ IEPs without consideration of a child’s individualized need for such services. All of the children at Manson get a relatively standard number of counseling hours each month, regardless of their need or the number of hours of counseling they received in their prior educational setting. For example, Manson reduced Christopher’s school-based counseling services by 80 percent. He went from receiving one hour and 15 minutes per week of counseling services in his local school district to just 15 minutes per week at Manson, notwithstanding that his IEP indicates concerns regarding “[i]nternalizing behaviors and coping skills” and notes that “[d]ue to [his] difficulty regulating his emotional control, he will need structured support in order to maintain progress in the general curriculum.” Manson similarly cut David’s counseling services by more than 87 percent. His counseling services went from two hours per week at his local school district to 15 minutes per week at Manson, even though his IEP indicates concerns regarding his “anger, frustration, impatience and anxiety,” and notes that due to his “difficulties sustaining attention, communicating his feelings, and low frustration tolerance, he requires a small structured setting with behavioral supports to be successful in the regular classroom.” Common modifications and accommodations specified in the IEPs of Manson students include extra time to complete lessons, hands on projects, cueing and prompting, vocabulary lists and study guides, assistance with organizational skills, peer support or mentoring, visuals to support instruction, daily feedback on behavior, and use of positive reinforcement. 22 In comparison to more than 60 percent of children at Manson qualifying for special education services, only about 14 percent of all public school students nationwide received special education services during the 2019-2020 school year. Véronique Irwin, Institute of Education Sciences, Report on the Condition of Education 2021 13, https://nces.ed.gov/pubs2021/2021144.pdf. 21 18 Likewise, Manson cut Christian’s counseling services by over 93 percent. Christian went from receiving five hours of counseling per week at his local school district to 20 minutes per week at Manson. These reductions were typical of the reductions in the IEPs developed at Manson. On average, children’s IEPs at Manson provided about 15 minutes per week of counseling services at Manson, as compared with over 70 minutes of services per week in the IEPs created by their local school districts. IEP Counseling Services (minutes per week) 80 60 40 20 0 Manson Home School District Manson also routinely reduces or eliminates children’s speech and language services. 23 For example, Nathan was receiving 30 minutes of speech and language services a week in his local school district, but received no speech and language services through his Manson IEP, which was developed less than six months later. The services were cut without explanation and despite the fact that the Manson IEP indicated that “all components of the [home school IEP] would be continued.” d. Manson Fails to Provide Adequate Behavioral Supports for Children with Disabilities IDEA requires that IEP teams consider developing positive behavioral interventions when a child’s “behavior impedes the child’s learning or that of others.” 20 U.S.C. § 1414(d)(3)(B)(i). To determine whether behaviors are impeding a child’s learning, schools frequently conduct functional behavioral assessments. These assessments are then used to create a behavior intervention plan to address the target behavior. At Manson, student behavior frequently interferes with classroom instruction. For example, in just one month, teachers issued at least 28 disciplinary tickets for behaviors such as disrupting class and not following directions. Seventy-five percent of these incidents involved students with identified disabilities, many of which can lead to distracting and disruptive 23 Even when children at Manson receive speech and language services, these services are not provided by a qualified speech and language pathologist. Instead, these services are provided by a special education teacher who is instructed to consult with a speech and language pathologist. Manson failed to provide any documentation regarding this consultation model and similarly failed to provide any documentation demonstrating whether and how speech and language services were provided under this model. Therefore, we cannot assess whether the provision of these services by someone other than a speech and language pathologist adequately meets the needs of students. 19 classroom behaviors when not properly addressed. As a result of these disciplinary tickets, the students lost recreation time and/or access to commissary for as long as seven days for a single incident. Still, no student at Manson had a functional behavioral assessment or a behavior intervention plan. For example, Christopher, a child with attention deficit hyperactivity disorder (ADHD), had a behavior support plan to address off-task behaviors and non-compliance with directives at his home school district. 24 At Manson, he did not have a behavior support plan and was disciplined four times in less than one month. 25 He was removed for movement in the classroom that was disruptive, not complying with instructions, and being disruptive in the class setting, which are typical characteristics of the behaviors of a child with ADHD. This resulted in a total of twelve days of loss of recreation and twelve days loss of commissary. Christian, a student classified with an emotional disturbance, was disciplined seven times in one year for aggressive threats, being extremely talkative in class, having side conversations in class, not following directions, and fighting. This resulted in a total of 4 days of Extended CTQ, 9 days High CTQ, 11 days moderate CTQ, 42 days of loss of recreation/low CTQ, and 21 days loss of commissary. Yet Manson did not develop a behavior support plan for Christian to address this conduct. 26 Manson also fails to conduct manifestation determinations when children are excluded from school for disciplinary reasons. Before a school can change the placement of a child with a disability (i.e., removal for more than 10 school days), it must conduct a “manifestation determination,” which is a review of all relevant information to determine if the questioned behavior was caused by, or had a direct and substantial relationship to, the child’s disability or the failure to implement the child’s IEP. 20 U.S.C. § 1415(k)(1)(E). Furthermore, if an education provider removes a student from the classroom for more than 10 days in a school year, it must provide the services necessary to allow the child “to continue to participate in the general education curriculum and to progress toward meeting the goals set out in the child’s IEP.” Id. § 1415(k)(1)(D)(i). USD #1 has taken the position that manifestation hearings are not required because custody staff, not school staff, are responsible for determining the length of time a child is sent to CTQ and removed from the classroom. But IDEA “protections apply regardless of whether a student who violates a code of student conduct is subject to discipline in the facility or removed Christopher also described that, under his prior IEP, he was allowed to take a break or go for a walk, if needed, as well as use headphones to do work. He said those options are not available at Manson, but would be helpful. 25 As described in previous sections of this Report, Manson also failed to adequately assess Christopher’s mental health needs and his special education services and counseling hours were dramatically reduced by Manson. 26 Similar to other students, Christian’s special education services were drastically reduced when he arrived at Manson (from 24.5 hours per week to two hours per week), and, as described above, his counseling services were cut by 91 percent. These services were cut without justification or consideration of how the reductions might impact his ability to productively and appropriately participate and engage in class. 24 20 to restricted settings, such as confinement to the student’s cell or ‘lockdown’ units.” 27 It is a violation of IDEA to remove children with disabilities from school for disciplinary reasons for more than 10 school days without conducting a manifestation determination or without providing special education and related services. Finally, although Manson purports to have a positive behavioral intervention system in which students may earn points for positive behavior, we found little evidence that this system is actually utilized by teachers. Classroom observations suggest that when students become disruptive, teachers are more likely to rely on out-of-school disciplinary consequences (e.g., loss of commissary or loss of recreation) to punish the students for in-school negative behaviors than employ positive behavior management techniques. In fact, multiple children complained about the number of “informals” or “tickets” that they received at school, often for minor misbehaviors. Samuel, a student with emotional disturbance, reported that he frequently would skip school rather than risk getting “informals,” which result in a loss of recreation time and access to commissary. He noted that he complained to his mental health therapist about the “informals,” but was told that they cannot help with that school issue. e. Manson Fails to Provide Adequate Transition Planning and Services For older children with disabilities, IDEA requires IEPs to include transition services that are “designed to . . . facilitate the child’s movement from school to post-school activities, including post-secondary education, vocational education, integrated employment . . . independent living, or community participation.” 34 C.F.R. § 300.43(a)(1). These transition services must include “appropriate measurable postsecondary goals based upon age appropriate transition assessments related to training, education, employment, and, where appropriate, independent living skills; [and] the transition services (including courses of study) needed to assist the child in reaching those goals.” 20 U.S.C. § 1414(d)(1)(A)(i)(VIII). Transition planning is particularly important for children with disabilities in correctional institutions, as they, overall, have poor post-release education and employment outcomes. Barriers to success may be particularly acute for students with disabilities who have arrests and/or convictions in the adult criminal justice system. Transition planning required by IDEA provides an opportunity to develop realistic post-secondary goals for the students incarcerated in Manson, and provide the services and supports to assist the students in reaching these goals. Many of the transition services offered by Manson, however, fail to provide the services and supports that would enable students to transition successfully from school to post-school activities. Many students are offered the same, relatively generic transition services (e.g., Letter from Melody Musgrove & Michael K. Yudin, U.S. Dep’t of Educ. 5 (Dec. 5, 2014), https://sites.ed.gov/idea/files/idea-letter. See also V.W. by & through Williams v. Conway, 236 F. Supp. 3d 554, 587 (N.D.N.Y. 2017) (finding plaintiffs demonstrated they are substantially likely to succeed on the merits of their IDEA claims where they alleged that “the routine use of solitary confinement . . . in response to behavioral issues” violates the manifestation hearing requirement of the IDEA and that the distribution of work packets to children with disabilities in solitary confinement violates the requirement that “the education provider must continue to provide the services necessary to ‘enable the child to continue to participate in the general education curriculum, although in another setting, and to progress toward meeting the goals set out in the child’s IEP.’”) (internal citations omitted). 27 21 completing career inventories, selection potential career paths, and writing reports on those potential careers), and the frequency of services is low. Notably, students in Manson’s high school program lacked access to hands-on vocational programming provided to the over 18 population. 2. Manson Fails to Meet Its “Child Find” Obligations Under the IDEA The “child find” provisions of IDEA require the State to implement “policies and procedures to ensure that” “[a]ll children with disabilities . . . who are in need of special education and related services[ ] are identified, located, and evaluated.” 34 C.F.R. § 300.111(a)(1)(i). Manson, however, lacks formal structures and procedures to ensure that children with disabilities are identified and evaluated. In 2019, Manson did not refer any students for evaluations to determine if they were in need of special education services. V. MINIMAL REMEDIAL MEASURES To remedy the constitutional and statutory violations identified in this Report, we recommend that Manson implement, at minimum, the remedial measures listed below. A. Isolation Manson should: 1. Prohibit the use of isolation with children for minor misbehaviors and when children pose no threat to safety. 2. Develop and implement a system for ensuring that children who are placed in isolation are returned to the general population as soon as they no longer pose a threat to safety. 3. Develop and implement a system for ensuring that children are not punished for behaviors related to mental illness or disabilities. 4. B. Replace the use of CTQ with a system for responding to children’s misbehaviors that relies on de-escalation and positive behavior management tools. Mental Health Care Manson should: 1. Provide adequate mental health intake screening and assessments, including adequate consideration of trauma-related mental health difficulties and the implications of dual diagnoses. 22 2. Provide adequate ongoing assessment of children’s mental health needs, including continued consideration of trauma-related mental health difficulties and the implications of dual diagnoses. 3. Provide adequate mental health treatment to children, including individual treatment and age-appropriate group therapy options. 4. Discontinue the practice of lowering children’s mental health scores based on non-compliance with a prescribed therapy or medication regimen. C. Special Education Services Manson should: 1. Provide individualized special education and related services, including transition services, to students with disabilities. 2. Implement modifications and accommodations required by student’s IEPs. 3. Provide adequate behavior interventions and supports for students with disabilities. 4. Utilize reliable screening processes and protocols to ensure the timely evaluation of children suspected of having a disability. VI. CONCLUSION The Department has reasonable cause to believe that Manson violates the constitutional and federal statutory rights of children by subjecting them to harmful isolation and failing to provide adequate mental health care and special education services. We look forward to working cooperatively with the State to reach agreement on the remedies for these violations. We are obligated to advise you that 49 days after issuance of this letter, the Attorney General may initiate a lawsuit pursuant to CRIPA to correct deficiencies identified in this letter if State officials have not satisfactorily addressed our concerns. 42 U.S.C. § 1997b(a)(1). The Attorney General may also move to intervene in related private suits 15 days after issuance of this letter. 42 U.S.C. § 1997c(b)(1)(A). Please also note that this Report is a public document. It will be posted on the Civil Rights Division’s website. 23