Bop Grievance Form 2002
Download original document:
Document text
Document text
This text is machine-read, and may contain errors. Check the original document to verify accuracy.
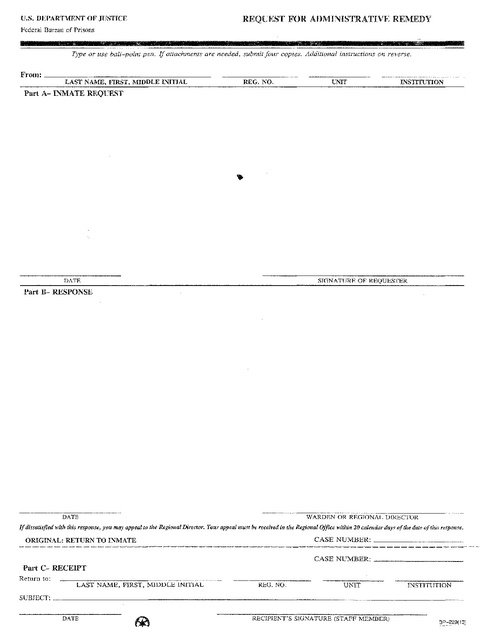
REQUEST FOR ADMINISTRATIVE REMEDY
U.S. DEPARTMENT OF JUSTICE
Federal Bureau of Prisons
Type or use
ball~poin{ pen.
If attachment,)' are needed, submit four copies. Additional instructions on reverse.
From:
_
LAST NAME,
I~IRST,
MIDDLE INITIAL
INSTITUTION
REG. NO.
Part A- INMATE REQUEST
SIGNATURE OF REQUESTER
DATE
Part B- RESPONSE
DATE
WARDEN OR REGIONAL DIRECTOR
If dissatisfied with this response, you may appeal to the Regional Director. Your appeal must be received in the Regional Office within 20 calendar days aithe date of this response.
ORIGINAL: RETURN TO INMATE
CASE NUMBER:
_
CASE NUMBER:
_
Part C- RECEIPT
Return to:
LAST NAME, FIRST. MIDDLE INITIAL
REG. NO.
UNIT
SUBJECT:
INSTITUTION
_
DATE
RECIPIENT'S SIGNATURE (STAFF MEMBER)